

Kidney transplantation is the management of choice in patients with end-stage chronic kidney disease. For decades it has been shown to offer improved quality of life and a lesser mortality risk compared with hemodialysis.1 However, transplantation remains a complex process and involves patients with important comorbidities. It is therefore essential to optimize the postoperative care of these individuals in the Intensive Care Unit (ICU). Imaging techniques play a very important role in this respect. Both renal doppler ultrasound (RDU) and radioisotopic studies (renal scintigraphy) are of great help in the identification of early complications, and afford very useful basal information for adequate graft assessment.2,3
Renal doppler ultrasound performed at the patient bedside by the intensivist makes it possible to discard acute complications such as bleeding, hydronephrosis, vascular dehiscence, arterial stenosis, venous thrombosis or renal infarction.2 The technique is moreover inexpensive, noninvasive and avoids the need for patient transfer. Furthermore, the renal resistance index (RI) (RI=peak systolic flow−end-diastolic flow/peak systolic flow) allows the quantification of graft flow alterations. It was originally used to diagnose acute rejection,4 though recently it has also been regarded as a chronic rejection marker.5 On the other hand, RI>0.8 has been shown to be a strong predictor of graft loss, being related to donor death.5 However, despite its prognostic value in transplant patients, RI is more closely related to recipient age and certain hemodynamic factors than to renal anomalies.6,7 Radioisotopic studies in turn allow evolutive monitoring of the graft. Although a single or point evaluation is unable to distinguish between acute tubular necrosis and acute rejection, serial radioisotopic studies evidencing a progressive decrease in function and perfusion could be indicative of acute rejection.8
In our ICU, renal doppler ultrasound is performed by the intensivist in the immediate postoperative period, while renal scintigraphy is routinely performed on the morning after the operation. In the event of an interval of more than 12h between both explorations, a new ultrasound study is made before patient transfer. Since our Unit provides support for a large number of kidney transplants, we decided to conduct a retrospective observational study, analyzing the explorations made between January 2013 and December 2015 in all patients admitted to the ICU in the immediate postoperative period of kidney transplantation. In this context, on performing RDU, adequate flow was defined as RI≤0.7 in the principal renal artery and in the segmental renal arteries. In relation to scintigraphy, mercaptoacetylglycine (MAG-3) is the radionuclide of choice in our center. The three phases of renal function were evaluated. The first phase shows graft perfusion based on images obtained during the first minute after intravenous injection of the tracer. The second phase evidences tracer extraction by the nephron and its excretion via glomerular filtration and/or tubular secretion. The third phase in turn assessed elimination of the tracer. Slight tubular dysfunction and/or a small delay in tracer elimination were considered normal.
A descriptive analysis was made, followed by comparison of the evolution of renal function in the transplant patients according to the type of donor involved. The Student's t-test was used in the presence of normal data distribution, while the Mann–Whitney U-test was applied in the absence of a normal distribution. The kappa test was used to assess agreement between the two flow tests used (RDU and scintigraphy). Statistical significance was considered for p<0.05. The SPSS version 22.0 statistical package (IBM Corporation, NY, USA) was used throughout.
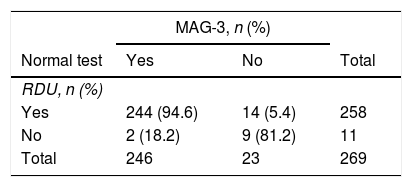
A total of 273 patients (60.1% males) were included during the study period. The mean age was 52 years. The patient characteristics are shown in Table 1, while agreement between the two tests is reported in Table 2 – the kappa index being 0.5 (p<0.001).
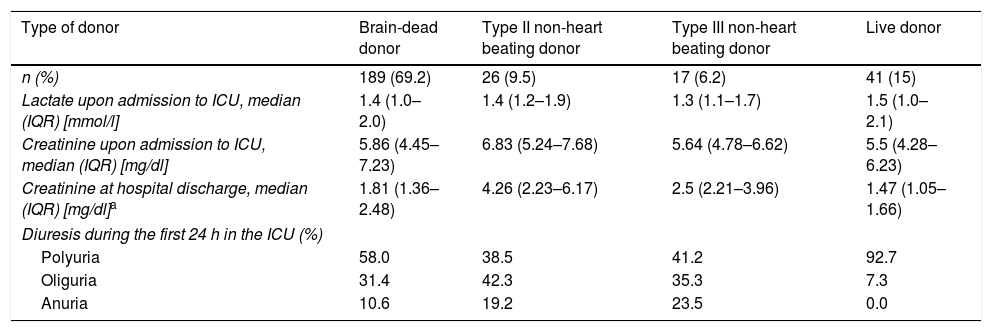
General characteristics of the kidney transplant patients.
| Type of donor | Brain-dead donor | Type II non-heart beating donor | Type III non-heart beating donor | Live donor |
|---|---|---|---|---|
| n (%) | 189 (69.2) | 26 (9.5) | 17 (6.2) | 41 (15) |
| Lactate upon admission to ICU, median (IQR) [mmol/l] | 1.4 (1.0–2.0) | 1.4 (1.2–1.9) | 1.3 (1.1–1.7) | 1.5 (1.0–2.1) |
| Creatinine upon admission to ICU, median (IQR) [mg/dl] | 5.86 (4.45–7.23) | 6.83 (5.24–7.68) | 5.64 (4.78–6.62) | 5.5 (4.28–6.23) |
| Creatinine at hospital discharge, median (IQR) [mg/dl]a | 1.81 (1.36–2.48) | 4.26 (2.23–6.17) | 2.5 (2.21–3.96) | 1.47 (1.05–1.66) |
| Diuresis during the first 24 h in the ICU (%) | ||||
| Polyuria | 58.0 | 38.5 | 41.2 | 92.7 |
| Oliguria | 31.4 | 42.3 | 35.3 | 7.3 |
| Anuria | 10.6 | 19.2 | 23.5 | 0.0 |
Few studies to date have compared RDU versus radioisotopic explorations for the evaluation of early graft function. Cofán et al.9 found that RDU did not discriminate the severity of graft acute tubular necrosis, while altered renogram findings were correlated to an increased need for hemodialysis and a decrease in graft survival. Another study in pediatric patients10 found renal blood flow as calculated from radioisotopic techniques to offer a more reliable assessment of graft dysfunction than RI measurement. A more recent study8 concluded that serial isotopic tests combined with kidney biopsy are more reliable in demonstrating graft dysfunction.
The great majority of specialized centers use both scintigraphy and RDU for evaluating the graft. However, in our study agreement (kappa index) with the perfusion indices was found to be moderate. Since most of the patients were admitted during hours on duty, RDU was performed by the intensivist available at the time. Although our team has extensive experience with transplants, the possible inter-observer effect of ultrasound could constitute a limitation in our study.
Kidney transplantation requires adequate postoperative care in order to guarantee good graft evolution in the first hours. In coincidence with other series, our results illustrate the early renal graft functional differences according to the type of donor involved. These differences are mainly due to the existence of longer warm ischemia times in the case of grafts harvested from type II non-heart beating donors. Nevertheless, it is known that these differences are minimized over the long term.11 In this regard, RDU and scintigraphy contribute very valuable information and have made it possible to maintain good functional outcomes in recent years. Our findings suggest that it is advisable to continue using both diagnostic tools for evaluating kidney transplants, integrating the results of these two tests in the clinical context of each individual patient.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Roldán-Reina AJ, Egea-Guerrero JJ, Palomo-López N, Cuenca-Apolo DX, Adriaensens-Pérez M, Martín-Villén L. Postoperatorio de trasplante renal en la unidad de cuidados intensivos: evaluación del injerto mediante técnicas de imagen. Med Intensiva. 2019;43:384–386.

