

Antiplatelet drugs play a key role in the management of ischemic heart disease and other diseases, exerting their effects though different pathways. The most useful of these drugs in application to coronary disease are the cyclooxygenase inhibitors: acetylsalicylic acid (ASA, aspirin), which is the most widely studied and used substance,1 and triflusal; and the P2Y12 antagonists: ticlopidine, clopidogrel, prasugrel and ticagrelor.
According to the current ischemic heart disease guides, in allergic patients were ASA is necessary, a rapid desensitization protocol must be applied,2 involving the administration of increasing doses of the drug until tolerance is achieved. Different rapid desensitization protocols have been described,3–5 with a duration of 2–5h, that can be used in unstable patients, with excellent efficacy and safety.
Despite the lack of clinical evidence to the effect (since no studies have suppressed the use of ASA), in patients who are hypersensitive to nonsteroidal antiinflammatory drugs and suffer confirmed chronic ischemic heart disease (detection of coronary atherosclerosis by computed axial tomography or positive ischemia testing), it is common to empirically prescribe triflusal or clopidogrel in monotherapy. In the event of percutaneous coronary intervention with the placement of a stent, even double-dose clopidogrel (or the prescription of prasugrel–ticagrelor) during one year has been used. In patients with acute coronary syndrome, dual antiplatelet treatment with triflusal and a P2Y12 inhibitor has been used on an empirical basis.
From the pharmacoeconomic perspective, ASA desensitization in patients with ischemic heart disease is comparatively less expensive in the context of both monotherapy and dual antiplatelet treatment (Tables 1 and 2).
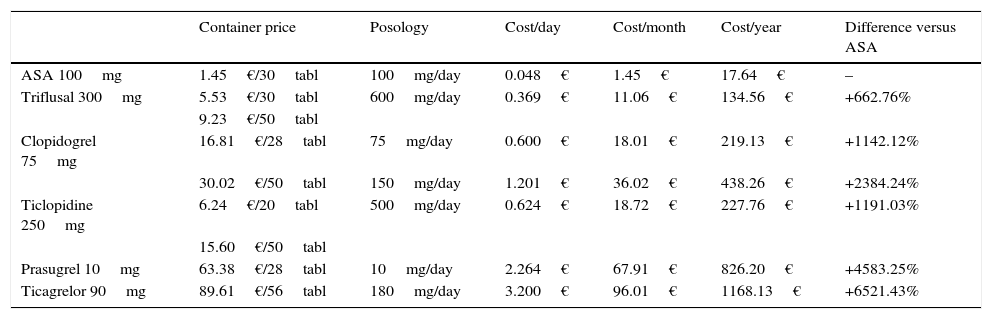
Prices and treatment costs of the different antiplatelet drugs.
| Container price | Posology | Cost/day | Cost/month | Cost/year | Difference versus ASA | |
|---|---|---|---|---|---|---|
| ASA 100mg | 1.45€/30tabl | 100mg/day | 0.048€ | 1.45€ | 17.64€ | – |
| Triflusal 300mg | 5.53€/30tabl | 600mg/day | 0.369€ | 11.06€ | 134.56€ | +662.76% |
| 9.23€/50tabl | ||||||
| Clopidogrel 75mg | 16.81€/28tabl | 75mg/day | 0.600€ | 18.01€ | 219.13€ | +1142.12% |
| 30.02€/50tabl | 150mg/day | 1.201€ | 36.02€ | 438.26€ | +2384.24% | |
| Ticlopidine 250mg | 6.24€/20tabl | 500mg/day | 0.624€ | 18.72€ | 227.76€ | +1191.03% |
| 15.60€/50tabl | ||||||
| Prasugrel 10mg | 63.38€/28tabl | 10mg/day | 2.264€ | 67.91€ | 826.20€ | +4583.25% |
| Ticagrelor 90mg | 89.61€/56tabl | 180mg/day | 3.200€ | 96.01€ | 1168.13€ | +6521.43% |
Prices referred to Spain and updated in August 2016.
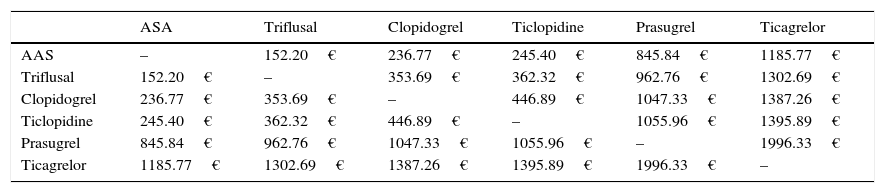
Annual cost per patient of the dual antiplatelet drug combinations.
| ASA | Triflusal | Clopidogrel | Ticlopidine | Prasugrel | Ticagrelor | |
|---|---|---|---|---|---|---|
| AAS | – | 152.20€ | 236.77€ | 245.40€ | 845.84€ | 1185.77€ |
| Triflusal | 152.20€ | – | 353.69€ | 362.32€ | 962.76€ | 1302.69€ |
| Clopidogrel | 236.77€ | 353.69€ | – | 446.89€ | 1047.33€ | 1387.26€ |
| Ticlopidine | 245.40€ | 362.32€ | 446.89€ | – | 1055.96€ | 1395.89€ |
| Prasugrel | 845.84€ | 962.76€ | 1047.33€ | 1055.96€ | – | 1996.33€ |
| Ticagrelor | 1185.77€ | 1302.69€ | 1387.26€ | 1395.89€ | 1996.33€ | – |
Prices referred to Spain and updated in August 2016.
In monotherapy, the annual cost of clopidogrel or triflusal is respectively 1142.12% (218.13 vs 17.64€) and 662.76% (134.56 vs 17.64€) greater than the cost of ASA. These differences could greatly increase (between 1408.05 and 3778.23%) in the case of treatment during the first 1–6months with prasugrel (cost between 266.02 and 515.52€) or ticagrelor (cost between 294.12 and 684.12€), followed by clopidogrel, as recommended by some guides.2
At present, the only dual antiplatelet treatment protocol recommended by the current guides is ASA plus a P2Y12 inhibitor.2 As a result, in patients allergic to ASA, desensitization to the latter drug is indicated for correct treatment, and this is moreover the least expensive option (Table 2). As an example, ASA plus clopidogrel has an annual cost per patient of 236.77€, which is far lower than in the case of the rest of the possible dual antiplatelet treatment combinations.
In conclusion, ASA is the option with the greatest supporting clinical evidence and lowest cost for the treatment of ischemic heart disease. Acetylsalicylic acid desensitization is required in patients who are allergic to the drug, indistinctly of whether it is prescribed as monotherapy or in the context of dual antiplatelet treatment. Close coordination is required among the Departments of Allergic Diseases, Cardiology and Intensive Care Medicine in order to develop protocols adapted to the needs of each center, with a view to optimizing the management of these patients.
Please cite this article as: Cubero JL, Simó Sánchez B, Millán P, Colás C. Desensibilización al ácido acetilsalicílico en pacientes con cardiopatía isquémica: ahorro de costes. Med Intensiva. 2017;41:446–447.

