
Infection during mechanical circulatory support is a frequent adverse complication. We analyzed infections occurring in this population in a national tertiary care center, and assessed the differences existing between the setting of extracorporeal membrane oxygenation (ECMO) and ventricular assist devices (VADs).
Design, setting, and participantsAn observational study was made of patients treated with ECMO or VAD in the San Raffaele Scientific Institute (Italy) between 2009 and 2011.
InterventionsNone.
ResultsThirty-nine percent of the 46 patients with ECMO and 69% of the 15 patients with VAD developed infection. We observed a mortality rate of 36.1% during mechanical circulatory support and of 55.7% during the global hospitalization period. Although Gram-negative infections were predominant overall, patients with ECMO were more prone to develop Candida infection (29%), and patients with VAD tended to suffer Staphylococcus infection (18%). Patients with infection had longer ECMO support (p=0.03), VAD support (p=0.01), stay in the intensive care unit (p=0.002), and hospital admission (p=0.03) than patients without infection.
Infection (regression coefficient=3.99, 95% CI 0.93–7.05, p=0.02), body mass index (regression coefficient=0.46, 95% CI 0.09–0.83, p=0.02), fungal infection (regression coefficient=4.96, 95% CI 1.42–8.44, p=0.009) and obesity (regression coefficient=10.47, 95% CI 1.77–19.17, p=0.02) were predictors of the duration of ECMO support. Stepwise logistic regression analysis showed the SOFA score at the time of implant (OR=12.33, 95% CI 1.15–132.36, p=0.04) and VAD (OR=1.27, 95% CI 1.04–1.56, p=0.02) to be associated with infection.
ConclusionsInfection is a major challenge during ECMO and VAD support. Each mechanical circulatory support configuration is associated with specific pathogens; fungal infections play a major role.
La infección es una complicación asociada habitualmente al soporte circulatorio mecánico. Analizamos las infecciones manifestadas en esta población en un centro de atención terciaria italiano y evaluamos las diferencias existentes entre la oxigenación con membrana extracorpórea (ECMO) y los dispositivos de asistencia ventricular (VAD).
Diseño, ámbito y participantesSe llevó a cabo un estudio observacional de pacientes tratados con ECMO o VAD en el Instituto Científico de San Raffaele (Italia) entre 2009 y 2011.
IntervencionesNinguna.
ResultadosEl 39 % de los 46 pacientes tratados con ECMO y el 69 % de los 15 pacientes tratados con VAD manifestaron una infección. Observamos una tasa de mortalidad del 36,1 % durante el soporte circulatorio mecánico y del 55,7 % durante el periodo de hospitalización global. Si bien en general las infecciones gramnegativas eran las predominantes, los pacientes con ECMO fueron más propensos a desarrollar infección por Candida (29 %), mientras que los pacientes tratados con VAD tendieron a sufrir infección por Staphylococcus (18 %). Los pacientes con infección recibieron más soporte con ECMO (p=0,03), más soporte con VAD (p=0,01), permanecieron durante más tiempo en la unidad de cuidados intensivos (p=0,002), y presentaron una tasa de ingreso hospitalario más elevada (p=0,03) que los pacientes que no sufrieron una infección.
Las infecciones (coeficiente de regresión=3.99, IC del 95 % 0,93-7,05, p=0,02), el índice de masa corporal (coeficiente de regresión=0.46, IC del 95 % 0,09-0,83, p=0,02), las infecciones micóticas (coeficiente de regresión=4,96, IC del 95 %C 1,42-8,44, p=0,009) y la obesidad (coeficiente de regresión=10,47, IC del 95 % 1,77-19,17, p=0,02) fueron factores predictivos de la duración del soporte con ECMO. Un análisis de la regresión logística escalonada mostró que la puntuación SOFA en el momento del implante (OR=12,33, IC del 95 % 1,15-132,36, p=0,04) y de la terapia con VAD (OR=1,27, IC del 95 % 1,04-1,56, p=0,02) se asociaban a infecciones.
ConclusionesLa infección representa un reto importante durante el soporte con ECMO y VAD. Cada configuración del soporte circulatorio mecánico se asocia a patógenos específicos; las infecciones micóticas desempeñan un papel importante.
The development of extracorporeal support devices has been fueled by the need to treat critically ill patients failing all conventional therapeutic options. In the last years, evidence regarding their safety and feasibility has grown, and their impact on the improvement of survival has also been demonstrated.1,2
In the setting of the intensive care unit, the most common types of extracorporeal support include extracorporeal membrane oxygenation (ECMO), and ventricular assist devices (VAD).
ECMO support is frequently percutaneous and not requiring surgery, but is associated with the need of bed riding, a larger exposure of blood to foreign surfaces, and, as it is used as a rescue therapy, with multiple organ damage. On the opposite, left VAD (LVAD) requires extensive surgery, and the tunneling of cannulas and drivelines through the chest of the patient. Furthermore, VAD is indicated in patients with preserved lung function, as the circuit does not include the oxygenator. Intracorporeal VAD is indicated in patients who are candidates to receive heart transplant or as destination therapy. On the contrary, paracorporeal VAD is employed for patients who could experience myocardial recovery.
Since the first experiences with prolonged extracorporeal support, infection has been unanimously pointed out as one of the most frequent and adverse complications.3–5
Indeed, infections occurring on extracorporeal support are often difficult to treat, especially if they involve the foreign device. Moreover, few data are available on the distribution and the penetration of antibiotics on their surfaces.
As both ECMO and VAD are increasingly used as a bridge to further therapeutic options, including heart and lung transplants, the presence of infection, however, jeopardizes patient's eligibility to receive these therapies, with consequent poor prognostic implications.
Despite the heavy burden of infection, paradoxically, few definite criteria and guidelines have been developed for the prevention and management of this complication during extracorporeal support. A marked variability in antimicrobial prophylaxis and infection surveillance practices among Extracorporeal Life Support Organization (ELSO) centers has also been reported.6
The different epidemiology of pathogens in the different intensive care units also contributes to make the task more difficult.
A comprehensive and rigorous picture of infection epidemiology, however, is the only basis on which protocols for infection prevention and management can be developed.
Aim of our study was to analyze rates and causal organisms of infections occurring in patients receiving ECMO or VAD, either paracorporeal or implantable, in a national tertiary referral center over a two-years period, and to assess the differences between these types of extracorporeal support setting.
Patients and methodsSetting and study populationThis study was conducted in the Cardiac Intensive Care Unit of San Raffaele Scientific Institute, in Milan, Italy. San Raffaele Scientific Institute is a teaching hospital and an Italian national tertiary referral center for extracorporeal support treatment.
The cardiac intensive care unit is a 14-bed adult critical care unit providing comprehensive care for critically ill patients undergoing cardiac surgery or with a primary cardiac diagnosis. Due to the presence of a trained team in extracorporeal support for the treatment of heart and lung failure, it was also elected as one of the 14 national tertiary referral centers of the Italian ECMOnet, a network created in 2009, to face the Italian H1N1 influenza A outbreak.5 Today, San Raffaele Scientific Institute is a referral center for venovenous (VV) ECMO, venoarterial (VA) ECMO, and VAD therapy.
Data collectionThe present study is in compliance with the Helsinki Declaration. After ethical committee approval, we collected data by chart review of inpatients records.
All adult patients receiving ECMO or VAD treatment and admitted to the Cardiac Intensive Care Unit of San Raffaele Scientific Institute between November 1, 2009 and October 31, 2011 were included in the study.
All data concerning patients’ demographic and comorbidities, hemodynamics, laboratory values, and outcome were analyzed. The presence or the absence of infections acquired during extracorporeal support was established, and the causal organisms registered.
Patients were followed until hospital discharge or death if occurring during hospitalization.
Inclusion and exclusion criteriaPatients were eligible for the present study if they were aged 18 or more and underwent ECMO or VAD between November 1, 2009 and October 31, 2011 at San Raffaele Scientific Institute in Milan.
Patients were excluded if the extracorporeal support lasted less than 48h. An infection acquired during extracorporeal support was defined as a culture proven infection from any site (i.e. blood, bronchoalveolar lavage specimen, deep tracheal aspirate, wound, urine) during ECMO or VAD support and not believed to be preexisting. In order to better differentiate infections acquired during bypass from those preexisting, cases with both a pre-extracorporeal support infection and an on-extracorporeal infection with the same organism were excluded.
In patients on ECMO or receiving VAD as a temporary support, the identified organism in question must have been recovered at least 24h after cannulation and within 7 days after ECMO or VAD discontinuation.
In patients receiving VAD as a destination therapy, we performed a follow-up of 3 months after implant for VAD-related infections identification, as this range was identified as the period with highest incidence of major infections in INTERMACS data registry.7
Accordingly, infections in patients with VAD were distinguished into VAD-specific infections, VAD-related infections, and non-VAD infections according to the criteria recently presented by the working formulation for the standardization of definitions of infections in patients using VAD.8
Extracorporeal devices and clinical managementThe ECMO circuit setup consisted of a centrifugal pump and a coated polymethylpentene oxygenator. For VV ECMO, either a femoro-jugular cannulation was performed, or a double-lumen dreinage and return cannula was employed. As for VA ECMO, a femorofemoral configuration of cannulas was adopted, and a distal perfusion cannula was inserted to prevent leg ischemia.
Treatment with VAD was either paracorporeal (either biventricular or monoventricular) or with fully implantable devices. Paracorporeal VAD circuit was identical to VA ECMO circuit, except for the absence of the oxygenator.
Continuous flow pumps were always used.
Different types of VADs were used: 4 patients received Levitronix Centrimag LVAD (2 LVAD and 2 BiVad (Levitronix LLC, Waltham, MA)), 2 received Incor LVAD (Berlin Heart Inc., Berlin, Germany), 3 had a Jarvik 2000 LVAD (Jarvik Heart Inc., New York, NY), 4 received Heart Mate II LVAD (Thoratec Corp., Pleasanton, CA), and 2 were implanted a HeartWare HVAD (HeartWare Inc., Miramar, FL).
All patients were intubated during ECMO support, except one patient who received VV ECMO after failure of non-invasive ventilation.
No microbiological sampling was routinely performed before initiation of the extracorporeal support, either ECMO or VAD.
As for infection surveillance and management, we followed international guidelines recommendations.9 Infection diagnosis followed CDC criteria for specific types of infections in the acute care setting.10
Three sets of blood cultures, deep tracheal aspirate or bronchoalveolar lavage, and urine samples were sent periodically to the laboratory for microbiological examination, and whenever deemed appropriate according to clinical practice.
Furthermore, when an intravascular device was changed or removed, the tip was sent for microbiological investigation.
The components of the ECMO circuit (including the oxygenator, the pump, and the cannulas) were never changed after infection identification.
All patients received intravenous continuous infusion of unfractionated heparin or bivalirudin titrated to maintain an activated partial thromboplastin time between 45 and 50s, gastric prophylaxis with histamine H2-receptor antagonists, hydration, and diuretics.
All patients received antibiotic prophylaxis with cephazolin for the first 48h after cannulation. No antifungal prophylaxis was routinely used. In patients already receiving antibiotics at ECMO initiation, the therapy was modified or maintained according to the decision of the medical attending team. The antibiotic therapy was always modified according to organ function, clinical situation, and culture results.
Statistical analysisCategorical variables are expressed as count (percentage), whereas continuous variables are shown as mean±standard deviation or as median and interquartile range if the standard deviation is larger than the mean in magnitude. Group comparison between infected and uninfected patients was performed using the nonparametric Mann–Whitney U test or Median test, and by Fisher's exact test, for continuous or categorical variables respectively. The rate of infection per 1000 days of ECMO and VAD was also calculated, and only the first episode of infection for each patient was taken into account in this analysis. A logistic regression analysis was carried out to detect the variables significantly associated with infection. A generalized linear model was used to identify predictors of the duration of ECMO or VAD support. The best multivariate model was selected by stepwise selection method of univariate significant covariates (univariate p value <0.25). A Kaplan–Meier curve and log-rank were performed to evaluate the difference of the time free from infection between the different types of support (VV ECMO, VA ECMO and VAD).
Statistical significance was set at the two-tailed 0.05 level for all hypothesis testing. Data were analysed with SAS 9.2 (SAS Institute Inc. Cary, NC, USA).
ResultsSeventy-five patients received extracorporeal support in the study period: 60 patients were treated with ECMO (37 VA ECMO and 23 VV ECMO), and 15 patients were implanted a VAD. Fourteen patients (13 on VA ECMO and 1 on VV ECMO) received extracorporeal support for less than 48h and were excluded from the analysis. Therefore 61 patients were included in our analysis: 46 patients treated with ECMO (24 with VA ECMO and 22 with VV ECMO) and 15 patients with VAD.
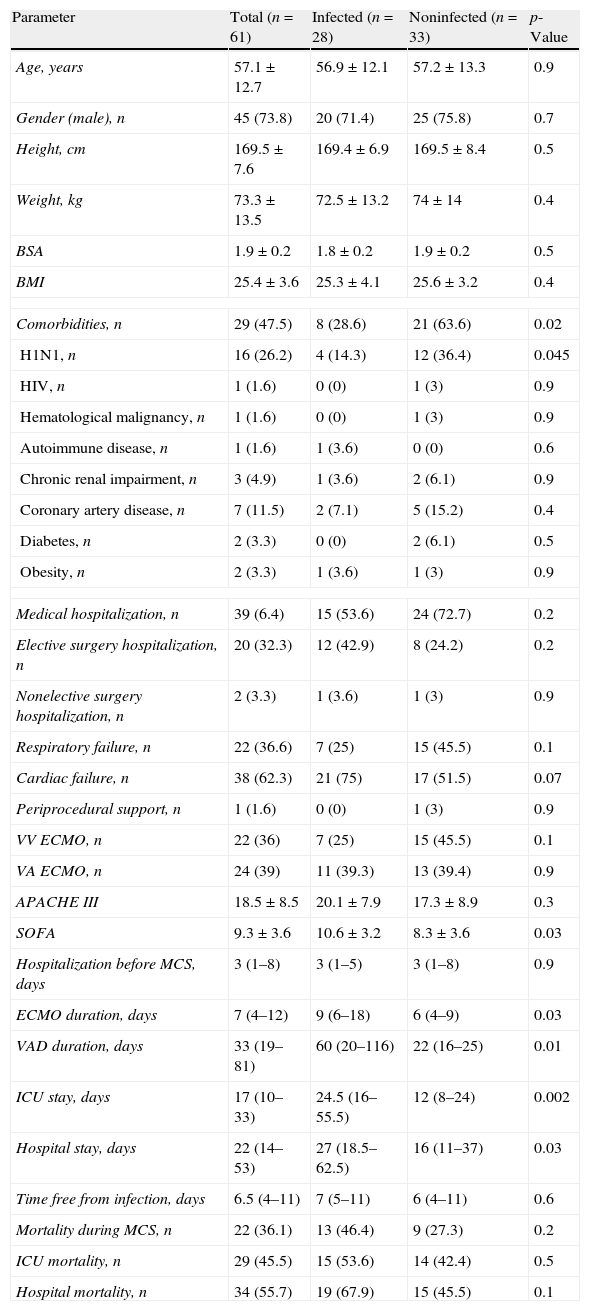
Patients’ characteristics, demographic and clinical data are shown in Table 1. Twenty-eight of the 61 patients (46%) developed extracorporeal related infection. Patients with infection had longer ECMO support duration (p=0.03), VAD support duration (p=0.01), intensive care unit (ICU) stay (p=0.002) and hospital stay (p=0.03) than patients without infection (p=0.03). Notably, patients with infection had a higher SOFA score at the time of implant than patients without infection (10.6±3.2 vs 8.3±3.6, p=0.03)
Patients’ characteristics, demographic and clinical data.
| Parameter | Total (n=61) | Infected (n=28) | Noninfected (n=33) | p-Value |
| Age, years | 57.1±12.7 | 56.9±12.1 | 57.2±13.3 | 0.9 |
| Gender (male), n | 45 (73.8) | 20 (71.4) | 25 (75.8) | 0.7 |
| Height, cm | 169.5±7.6 | 169.4±6.9 | 169.5±8.4 | 0.5 |
| Weight, kg | 73.3±13.5 | 72.5±13.2 | 74±14 | 0.4 |
| BSA | 1.9±0.2 | 1.8±0.2 | 1.9±0.2 | 0.5 |
| BMI | 25.4±3.6 | 25.3±4.1 | 25.6±3.2 | 0.4 |
| Comorbidities, n | 29 (47.5) | 8 (28.6) | 21 (63.6) | 0.02 |
| H1N1, n | 16 (26.2) | 4 (14.3) | 12 (36.4) | 0.045 |
| HIV, n | 1 (1.6) | 0 (0) | 1 (3) | 0.9 |
| Hematological malignancy, n | 1 (1.6) | 0 (0) | 1 (3) | 0.9 |
| Autoimmune disease, n | 1 (1.6) | 1 (3.6) | 0 (0) | 0.6 |
| Chronic renal impairment, n | 3 (4.9) | 1 (3.6) | 2 (6.1) | 0.9 |
| Coronary artery disease, n | 7 (11.5) | 2 (7.1) | 5 (15.2) | 0.4 |
| Diabetes, n | 2 (3.3) | 0 (0) | 2 (6.1) | 0.5 |
| Obesity, n | 2 (3.3) | 1 (3.6) | 1 (3) | 0.9 |
| Medical hospitalization, n | 39 (6.4) | 15 (53.6) | 24 (72.7) | 0.2 |
| Elective surgery hospitalization, n | 20 (32.3) | 12 (42.9) | 8 (24.2) | 0.2 |
| Nonelective surgery hospitalization, n | 2 (3.3) | 1 (3.6) | 1 (3) | 0.9 |
| Respiratory failure, n | 22 (36.6) | 7 (25) | 15 (45.5) | 0.1 |
| Cardiac failure, n | 38 (62.3) | 21 (75) | 17 (51.5) | 0.07 |
| Periprocedural support, n | 1 (1.6) | 0 (0) | 1 (3) | 0.9 |
| VV ECMO, n | 22 (36) | 7 (25) | 15 (45.5) | 0.1 |
| VA ECMO, n | 24 (39) | 11 (39.3) | 13 (39.4) | 0.9 |
| APACHE III | 18.5±8.5 | 20.1±7.9 | 17.3±8.9 | 0.3 |
| SOFA | 9.3±3.6 | 10.6±3.2 | 8.3±3.6 | 0.03 |
| Hospitalization before MCS, days | 3 (1–8) | 3 (1–5) | 3 (1–8) | 0.9 |
| ECMO duration, days | 7 (4–12) | 9 (6–18) | 6 (4–9) | 0.03 |
| VAD duration, days | 33 (19–81) | 60 (20–116) | 22 (16–25) | 0.01 |
| ICU stay, days | 17 (10–33) | 24.5 (16–55.5) | 12 (8–24) | 0.002 |
| Hospital stay, days | 22 (14–53) | 27 (18.5–62.5) | 16 (11–37) | 0.03 |
| Time free from infection, days | 6.5 (4–11) | 7 (5–11) | 6 (4–11) | 0.6 |
| Mortality during MCS, n | 22 (36.1) | 13 (46.4) | 9 (27.3) | 0.2 |
| ICU mortality, n | 29 (45.5) | 15 (53.6) | 14 (42.4) | 0.5 |
| Hospital mortality, n | 34 (55.7) | 19 (67.9) | 15 (45.5) | 0.1 |
BSA, body surface area; BMI, body mass index; HIV, human immunodeficiency virus; VV ECMO, venovenous extracorporeal membrane oxygenation; VA ECMO, venoarterial membrane oxygenation; LVAD, left ventricular assist device; BiVAD, biventricular assist device; ICU, intensive care unit; MCS, mechanical circulatory support.
Overall hospital mortality was 55.7%. Although patients with infection died more often than patients without infection (67.9% vs 45.5%), the difference in mortality did not reach a statistical significance (p=0.1).
The rate of infection was 57 per 1000 days of ECMO, 41 per 1000 days of VAD, and 50 per 1000 days mechanical circulatory support (i.e. ECMO and VAD considered all together).
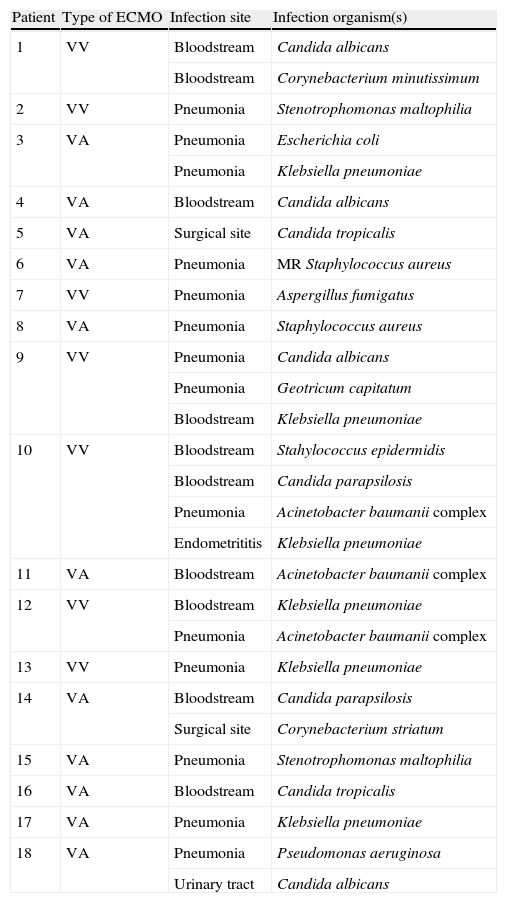
The overview of infections occurring in patients treated with ECMO is presented in Table 2.
Infections’ overview in patients treated with ECMO.
| Patient | Type of ECMO | Infection site | Infection organism(s) |
| 1 | VV | Bloodstream | Candida albicans |
| Bloodstream | Corynebacterium minutissimum | ||
| 2 | VV | Pneumonia | Stenotrophomonas maltophilia |
| 3 | VA | Pneumonia | Escherichia coli |
| Pneumonia | Klebsiella pneumoniae | ||
| 4 | VA | Bloodstream | Candida albicans |
| 5 | VA | Surgical site | Candida tropicalis |
| 6 | VA | Pneumonia | MR Staphylococcus aureus |
| 7 | VV | Pneumonia | Aspergillus fumigatus |
| 8 | VA | Pneumonia | Staphylococcus aureus |
| 9 | VV | Pneumonia | Candida albicans |
| Pneumonia | Geotricum capitatum | ||
| Bloodstream | Klebsiella pneumoniae | ||
| 10 | VV | Bloodstream | Stahylococcus epidermidis |
| Bloodstream | Candida parapsilosis | ||
| Pneumonia | Acinetobacter baumanii complex | ||
| Endometrititis | Klebsiella pneumoniae | ||
| 11 | VA | Bloodstream | Acinetobacter baumanii complex |
| 12 | VV | Bloodstream | Klebsiella pneumoniae |
| Pneumonia | Acinetobacter baumanii complex | ||
| 13 | VV | Pneumonia | Klebsiella pneumoniae |
| 14 | VA | Bloodstream | Candida parapsilosis |
| Surgical site | Corynebacterium striatum | ||
| 15 | VA | Pneumonia | Stenotrophomonas maltophilia |
| 16 | VA | Bloodstream | Candida tropicalis |
| 17 | VA | Pneumonia | Klebsiella pneumoniae |
| 18 | VA | Pneumonia | Pseudomonas aeruginosa |
| Urinary tract | Candida albicans |
ECMO, extracorporeal membrane oxygenation; VV, venovenous; VA, venoarterial; MR, Methicillin resistant.
Eighteen out of the 46 patients supported with ECMO (39%) developed nosocomial ECMO-related infection: 7 patients with VV ECMO, and 11 patients with VA ECMO.
Four of the 18 patients with infection (22%) developed a polymicrobial infection. In particular, 28 micro-organism were isolated: 13 Gram-negative bacteria (46%), 10 fungi (36%), and 5 Gram-positive bacteria (18%).
The most frequent pathogens responsible for infection were Candida spp. (29%), followed by Klebsiella spp. (21%).
Pneumonia was the most frequent type of infection (11 episodes), followed by bloodstream infection (8 episodes), surgical site infection (2 episodes), and urinary tract infection (1 episode).
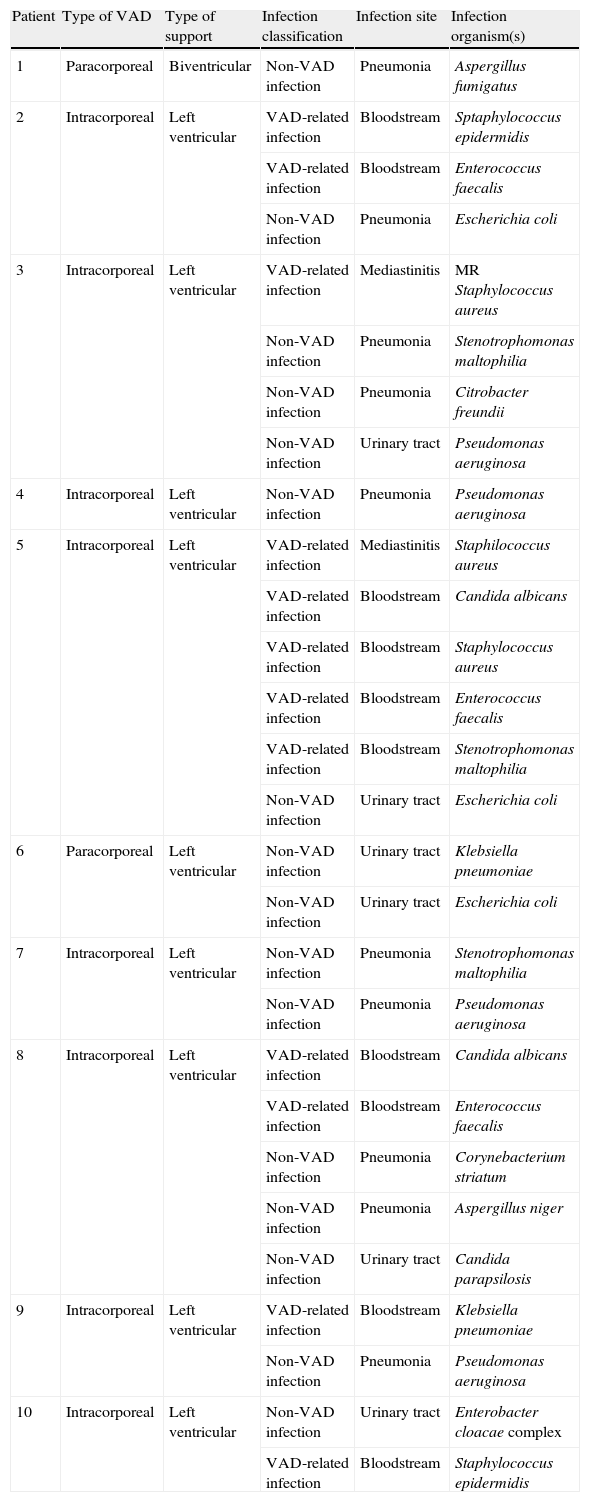
Micro-organisms responsible for infection in patients with VAD are listed in Table 3. Ten out of 15 patients (67%) developed nosocomial infection following VAD implantation, and 28 isolates were recorded: 14 Gram-negative bacteria (50%), 9 Gram-positive bacteria (32%), and 5 fungi (18%).
Infections’ overview in patients treated with VAD.
| Patient | Type of VAD | Type of support | Infection classification | Infection site | Infection organism(s) |
| 1 | Paracorporeal | Biventricular | Non-VAD infection | Pneumonia | Aspergillus fumigatus |
| 2 | Intracorporeal | Left ventricular | VAD-related infection | Bloodstream | Sptaphylococcus epidermidis |
| VAD-related infection | Bloodstream | Enterococcus faecalis | |||
| Non-VAD infection | Pneumonia | Escherichia coli | |||
| 3 | Intracorporeal | Left ventricular | VAD-related infection | Mediastinitis | MR Staphylococcus aureus |
| Non-VAD infection | Pneumonia | Stenotrophomonas maltophilia | |||
| Non-VAD infection | Pneumonia | Citrobacter freundii | |||
| Non-VAD infection | Urinary tract | Pseudomonas aeruginosa | |||
| 4 | Intracorporeal | Left ventricular | Non-VAD infection | Pneumonia | Pseudomonas aeruginosa |
| 5 | Intracorporeal | Left ventricular | VAD-related infection | Mediastinitis | Staphilococcus aureus |
| VAD-related infection | Bloodstream | Candida albicans | |||
| VAD-related infection | Bloodstream | Staphylococcus aureus | |||
| VAD-related infection | Bloodstream | Enterococcus faecalis | |||
| VAD-related infection | Bloodstream | Stenotrophomonas maltophilia | |||
| Non-VAD infection | Urinary tract | Escherichia coli | |||
| 6 | Paracorporeal | Left ventricular | Non-VAD infection | Urinary tract | Klebsiella pneumoniae |
| Non-VAD infection | Urinary tract | Escherichia coli | |||
| 7 | Intracorporeal | Left ventricular | Non-VAD infection | Pneumonia | Stenotrophomonas maltophilia |
| Non-VAD infection | Pneumonia | Pseudomonas aeruginosa | |||
| 8 | Intracorporeal | Left ventricular | VAD-related infection | Bloodstream | Candida albicans |
| VAD-related infection | Bloodstream | Enterococcus faecalis | |||
| Non-VAD infection | Pneumonia | Corynebacterium striatum | |||
| Non-VAD infection | Pneumonia | Aspergillus niger | |||
| Non-VAD infection | Urinary tract | Candida parapsilosis | |||
| 9 | Intracorporeal | Left ventricular | VAD-related infection | Bloodstream | Klebsiella pneumoniae |
| Non-VAD infection | Pneumonia | Pseudomonas aeruginosa | |||
| 10 | Intracorporeal | Left ventricular | Non-VAD infection | Urinary tract | Enterobacter cloacae complex |
| VAD-related infection | Bloodstream | Staphylococcus epidermidis |
VAD, ventricular assist device; MR, Methicillin resistant.
Seven out of the 10 patients with infection (70%) had a polymicrobial infection. Twelve micro-organisms were isolated in the context of a VAD-related infection, while the remaining 16 were responsible for non-VAD infections. No VAD-specific infection was observed.
The most frequently involved micro-organisms were Staphylococcus spp. (18%), and Pseudomonas aeruginosa (14%). In contrast to the epidemiology of ECMO-related infections, Candida spp. were found only in the 11% of the infective episodes.
Pneumonia was the most common type of infection in patients supported with VAD (7 episodes), followed by bloodstream infection (5 episodes), urinary tract infection (5 episodes), and mediastinitis (2 episodes).
In the total of patients undergoing mechanical support, Candida spp. were the predominant pathogens, as they were isolated in 11 episodes (20%).
SOFA score (OR=12.33, 95% CI 1.15–132.36, p=0.04) and VAD support (OR=1.27, 95% CI 1.04–1.56, p=0.02) were shown to be significantly associated with infection at logistic stepwise regression analysis. Gram-negative bacteria infections were associated with VAD support analysis (OR=4.11, 95% CI 1.20–14.12, p=0.02).
Moreover, independent significant predictors of the duration of ECMO support were the following: infection (regression coefficient=3.99, 95% CI 0.93–7.05, p=0.02), BMI (regression coefficient=0.46, 95% CI 0.09–0.83, p=0.02), fungal infection (regression coefficient=4.96, 95% CI 1.42–8.44, p=0.009), and obesity (regression coefficient=10.47, 95% CI 1.77–19.17, p=0.02).
The Kaplan–Meyer curves of time free from infection were not significantly different between the 3 groups (VV ECMO, VA ECMO, and VAD (p=0.2), between ECMO, either VV or VA, and VAD (p=0.2), and between VA ECMO and VAD (p=0.08)).
DiscussionOur study shows that infection is a very common complication in patients undergoing extracorporeal support. This is not surprising, as patients requiring ECMO or VAD support are a sick population of immunocompromised hosts with underlying comorbidities, often undergoing prolonged hospitalization and multiple drug regimens. Nevertheless, the inter-hospital comparison between different types and the incidence of infections in patients undergoing extracorporeal support have been limited by the fact that publications available on this topic were based on heterogeneous definitions of ECMO related and VAD related infections. Furthermore, micro-organisms’ epidemiology greatly varies among different intensive care units.
Patients or candidates to receive such therapies should not be regarded as a homogeneous category. Indeed, we observed a remarkable difference in infection rates and causal organisms between ECMO and VAD patients.
Incidence of infections occurring during ECMO treatment in literature ranges from 3.5% to 45.1%.11–15
In a query recently conducted on the 20,741 ECMO patients of the Extracorporeal Life Support Organization (ELSO), adult patients were found to be more vulnerable to infection compared to neonatal and pediatric population (infection rate of 30.6 per 1000 days of ECMO) with Candida spp being the predominant pathogen in the adult population, being responsible for 15% of infections.3
Furthermore, Sun et al. found that bloodstream infection is the most common infection, with Candida spp, Stenotrophomonas maltophilia, and Pseudomonas aeruginosa being the predominant blood isolates.16
Similarly, we confirmed that fungal infection is a frequent complication of ECMO, and we also found that it is associated with a longer duration of the ECMO support. Indeed, we showed that a high incidence of infections by Candida species was found in various studies, and that antimicrobial prophylaxis differs between centers as no guidelines exist.6
The incidence of Candida spp. infections that we reported in our population of patients supported with ECMO (29%) is higher compared to the 15% of the patients included in the ELSO registry.3 This observation further strengthens the consideration that the same pathogen may have a different impact in different clinical settings. The mortality attributable to Candida infection is known to be high in literature, ranging from 5% up to 49% according to the different types of studies (retrospective vs prospective), patients (ICU vs. non-ICU, comorbidity), and healthcare settings.17–19 Whether Candida spp. infection may play an impact on mortality also in ECMO patients is an intriguing issue, but we cannot answer this question based on our data, as we observed no statistically significant difference in mortality between patients with and without infection and due to the small sample size of our population.
VAD support too has been demonstrated to be associated with a high rate of both device-correlated and not device-correlated infection, the most feared being endovascular infection which is associated with increased mortality.20–22 In particular, Gordon et al. reported a bloodstream infection rate of 7.9 per 1000 VAD days.21
Recently, a multidisciplinary working group of the International Society for Heart and Lung Transplantation (ISHLT) provided a panel of standard international definitions including not only major infections but also comprehensive details of all aspects of VAD-specific and VAD-related infection in these patients.8
Therefore, we classified infection occurring in the patients of our study according to their definitions, which distinguish between VAD-specific, VAD-related, and non-VAD infections.
Interestingly, we did not observe VAD-specific infections during hospital stay, or at the 3-months follow-up. VAD-specific infections are a severe complication with a significant impact on the prognosis, but do not occur early after VAD implantation in our experience. On the contrary, we found that more than a half of patients receiving VAD support developed nosocomial infection before hospital discharge. The consequences of such infections on the prognosis of the patients and of the VAD, together with the costs of prolonged ICU and hospital stay, have probably been underestimated in the past. Notably, patients with paracorporeal VAD resulted to be less prone to develop infection than those with implantable devices in our experience, as no VAD-related infection was registered.
Gram-positive bacteria have been found to be the predominant pathogens responsible for infection in patients with VAD,23 and Staphylococcus species were the predominant pathogens also in our study population. However, VAD support was found to be associated with an increased occurrence of infections Gram-negative pathogens in our analysis, thus confirming that the burden of Gram-negative bacteria infection remains heavy also in these patients.
It should be also noticed that we reported a higher infection rate as compared to previous studies concerning mechanical circulatory support. The difference observed may have different explanations, including a slight heterogeneity of infection definition among different centers, bias in data collection, and a different degree of experience of different centers in dealing with patients treated with mechanical circulatory support which leads to a different incidence of complications.
Despite the few data available on this topic, however, all these studies show that infection is to be considered a very common complication during mechanical circulatory support.
Furthermore, patients with extracorporeal related infection require longer ICU stay and hospital stay than patients without infection, with subsequent consequent increasing costs. As a consequence, the need for prolonged antimicrobial therapies may lead to organ toxicity and the development of resistant microbiological strains. This phenomenon is also exacerbated by the fact that in the real world of ECMO and VAD it is difficult to discriminate as which patients are free from infection without any doubt, and, as a consequence, antibiotics are extensively used.
In the light of the data shown, we changed antimicrobial prophylaxis in patients undergoing mechanical circulatory support and we now routinely administer broad spectrum antibiotics and fluconazole.
However, the identification of the optimal prophylaxis for ECMO treatment is not trivial, as no randomized trials have ever addressed this issue.
A recent survey among ECMO centers6 reported that forty-two percent of centers routinely administer antibacterial prophylaxis to all ECMO patients. Among centers with standardized protocol or antibacterial prophylaxis based on physician preference, less than half use a single agent. On the contrary, only a minority of centers reported administering routine (2%) or selective antifungal agents (13%) to ECMO patients.
This study presents some limitations. First of all, we report data from a relatively small population of heterogeneous patients. Second, all data came from a single center. Third, patients usually received antibiotic prophylaxis and this might have influenced our results.
In conclusion, mechanical circulatory support related infections are frequent, difficult to treat, and lead to prolonged hospitalization. The epidemiology of infection is different among ECMO and VAD, suggesting the need for an appropriate antibiotic prophylaxis according to the type of extracorporeal support.
FundingThe work was supported by departmental funds.
Conflicts of interestThe authors have no conflicts of interest to declare.