

Adverse events significantly impact upon mortality rates and healthcare costs.
PurposeTo design a checklist of safety measures based on relevant scientific literature, apply random checklist measures to critically ill patients in real time (safety audits), and determine its utility and feasibility.
MethodsA list of safety measures based on scientific literature was drawn up by investigators. Subsequently, a group of selected experts evaluated these measures using the Delphi methodology. Audits were carried out on 14 days over a period of one month. Each day, 50% of the measures were randomly selected and measured in 50% of the randomized patients. Utility was assessed by measuring the changes in clinical performance after audits, using the variable improvement proportion related to audits. Feasibility was determined by the successful completion of auditing on each of the days on which audits were attempted.
ResultsThe final verified checklist comprised 37 measures distributed into 10 blocks. The improvement proportion related to audits was reported in 83.78% of the measures. This proportion was over 25% in the following measures: assessment of the alveolar pressure limit, checking of mechanical ventilation alarms, checking of monitor alarms, correct prescription of the daily treatment orders, daily evaluation of the need for catheters, enteral nutrition monitoring, assessment of semi-recumbent position, and checking that patient clinical information is properly organized in the clinical history. Feasibility: rounds were completed on the 14 proposed days.
ConclusionsAudits in real time are a useful and feasible tool for modifying clinical actions and minimizing errors.
Los eventos adversos impactan significativamente en la mortalidad y costes sanitarios.
ObjetivosElaborar un listado de verificación de medidas de seguridad basadas en la literatura científica más relevante, aplicarlo en tiempo real y aleatoriamente (rondas de seguridad) y determinar su utilidad y factibilidad.
DiseñoLos investigadores desarrollaron un listado de medidas de seguridad basado en la literatura científica. Posteriormente, mediante el método Delphi un grupo de expertos consensuaron las medidas. Las auditorías fueron realizadas en 14 días durante un mes. Cada día se seleccionaron aleatoriamente el 50% de las variables y se midieron en el 50% de los pacientes. La utilidad se determinó midiendo las modificaciones en la actuación clínica usando la variable «proporción de mejora relacionada con las auditorías». La factibilidad fue determinada por la capacidad de realizar los análisis cada día que fueron previstos.
ResultadosEl listado de verificación estuvo formado por 37 medidas distribuidas en 10 bloques. En el 83,78% de las medidas se produjeron modificaciones después de las rondas. La proporción de mejora relacionada con las rondas fue superior al 25% en las siguientes medidas: evaluación del límite de presión alveolar, revisión de las alarmas de la ventilación mecánica, revisión de las alarmas del monitor, prescripción correcta de las órdenes de tratamiento, evaluación diaria de la necesidad de catéteres, monitorización de la nutrición enteral, posición semiincorporada e información clínica del paciente. Factibilidad: las rondas fueron completadas los 14 días que se propusieron.
ConclusionesLas rondas de seguridad aleatorizadas son una herramienta útil y factible para modificar actuaciones clínicas minimizando los errores.
It is known that the occurrence of adverse events significantly impacts on mortality rates and health costs.1 Therefore, clinical safety is a priority in care.2–4
The critically ill patient is complex and frequently demands for the implementation of a great number of decisions and procedures in short periods of time. This increases the likelihood of errors, and therefore adverse events.5 Although errors, categorized as those of commission or those of omission,6 can be made anywhere in the hospital, critical care patients are among those least able to withstand the consequences of a mistake.7 Recent studies have highlighted the presence of multiple errors in intensive care. For example, Garrouste-Orgeas et al.8 reported that adverse events in the intensive care unit (ICU) have considerable prognostic significance, with a threefold increase in mortality among patients who experience more than two such events. Furthermore, Valentin et al.9 conducted a cross-sectional, observational study, carried out over 24h in 205 ICUs, in which 39 adverse events were described per 100 patients per day. Organ failure, a greater intensity in level of care and time of exposure were all related to these events. The same group10 reported that more than half of the errors were classified as errors of omission. These errors, usually less visible, may be associated to increased morbidity and mortality and are usually related to a lack of adherence to recommendations made based on scientific evidence. Often, in the critical care setting, there is a discrepancy between these recommendations and clinical practice.11 In Spain, the SYREC12 study also reported an increased risk of incidents in patients admitted to ICU (no-harm events and adverse events). Most incidents were considered avoidable.
Several methods have been described involving critical care patients to detect adverse events, ranging from the use of observers,13 to self-reporting systems or retrospective chart reviews.14 These methods tend to focus on the presence of adverse events and are not sensitive for routine monitoring of the areas of care where errors are most likely to occur.15,16 Some authors have investigated alternative, proactive methods for analysing the safety of critical patients.17 Such a methodology, which is less time consuming and provides rapid feedback, allows for immediate changes in practice where it might be necessary.
The main objectives of this study were to develop a checklist of safety measures (SMs) specifically designed for critically ill patients and based on sound scientific literature, and to apply them in real time (randomizing variables and patients) during routine clinical work (audits), with the aim of minimizing errors of both commission and omission, and evaluating the utility and feasibility of the procedure.
Patients and methodsThe Ethics Committee of the Hospital Universitari Joan XXIII in Tarragona approved the study, considering also that written informed consent by a patient could be waived for participation in the study.
Two sections can be differentiated: (1) Design of the checklist. (2) Pilot study and evaluation of utility and feasibility.
Design of the checklistDesign of the initial list of SMsA literature search was conducted using the MEDLINE (1990–Present – English and Spanish language articles) database. The following combined search MeSH terms were used: critical care, mechanical ventilation, haemodynamic monitoring, fluid balance, acute renal failure, sedation, analgesia, treatment, prevention, thromboembolic disease, gastrointestinal bleeding, hyperglycaemia, transfusion, nutrition monitoring, nursing care and quality indicators. Moreover, international and national guidelines, monographs and books in nursing literature concerning with standards of care and good clinical practice were reviewed. The most relevant bibliography is included in Appendix B. The selected measures based on this literature review had to comply with the following characteristics: designed to prevent errors of omission or commission, easily evaluable by a clinician in the course of the daily clinical visit; immediate applicability of the information derived from its evaluation allowing the modification of the patient care.
Initially, the SMs were distributed into nine blocks, as follows: (1) Mechanical Ventilation, (2) Haemodynamics, (3) Renal Function/Continuous Renal Replacement Techniques (CRRT), (4) Analgesia/Sedation, (5) Treatment, (6) Techniques and tests, (7) Nutrition, (8) Nursing Care, and (9) Structure. The structuring of the list of measures was as described by Hales et al.18
The Delphi processSubsequently, a group of experts were selected to perform an initial evaluation of the SMs using the Delphi method.19–25 Experts were selected from a group of critical care specialists and experienced nurses from both clinical care and research fields and were considered as referees on the study areas by the Spanish Society of Intensive and Coronary Care. Experts were invited to comment on each SM as well as to suggest other SMs that could be included in the checklist. Three rounds were considered enough to reach adequate consensus (Appendix C: Delphi method). Importance and feasibility of each item was rated using a 7-point scale, ranging from “not at all important” to “very important”, and “not at all feasible” to “very feasible” respectively. An SM was excluded at each stage if its rating was polarized to the extremes of the scale (that is, if three or more experts gave a high rating of 6 or 7 while, on the other hand, three or more gave a low rating of 1 or 2).25 Furthermore, cumulative percentage scores were then used to determine which of the remaining SMs met the inclusion criteria, that is, at least 80% of the expert panel giving an importance rating of 5 or more and a feasibility rating of 4 or more. Experts’ comments were carefully considered and they were given the opportunity to later request the reintroduction of any previously excluded item. Each SM contains a concept, inclusion criteria and an evaluation method.
Pilot study and evaluation of utility and feasibilityAudits in real time for safety in critical care (ART-SACC) procedureSMs were selected randomly from a checklist and applied during a clinical visit, at the bedside and in real time, to a number of patients who were also randomly selected. When applying ART-SACC, possible answers were as follows:
- 1.
Yes: the SM described was being carried out before the evaluation.
- 2.
Yes, after ART-SACC: the SM described was not being carried out before and, through ART-SACC, clinical practice was changed.
- 3.
No: the SM described was not being carried out before and, despite ART-SACC, clinical practice was not changed.
- 4.
Evaluation not applicable: the SM described was not analyzed because the patient did not meet the inclusion criteria specified (Appendix D: Variables that have been subjected to a Delphi method and included in the final checklist: concept, inclusion criteria and evaluation method).
The pilot study was conducted at University Hospital Joan XXIII of Tarragona, Spain, a tertiary hospital of 346 beds, which has a medical-surgical ICU department (without coronary patients) with 14 beds. Audits were conducted for a total of 14 days over a 30-day period. During this period there were no significant changes in medical and nursing staff. The nurse/patient ratio was 1:2. In our ICU, a senior intensive care doctor and a resident visit each patient.
Audits were carried out three days a week (Monday, Wednesday and Friday). All the ICU patients were considered for analysis. On each day of analysis half of the patients and half of the SMs were selected randomly, in order to minimize the time spent on the study. Staff were made aware when audits would be taking place but not on which patients or what SMs would be evaluated. Audits were carried out at bedside and, as a rule, the doctors, nurses and supervisor responsible for care were present at the evaluation moment, together with at least one of the researchers, who asked the questions.
Data routinely collected for each day of analysis included the following items: Sequential Organ Failure Assessment (SOFA), nurse/patient ratio, doctor/patient ratio, patients’ length of stay and the type of patient (medical, traumatic, surgical and neurosurgical). Responses were collected in a standardized way on a form designed for the purpose.
Utility and feasibility of ART-SACCUtility was evaluated from the proportion of changes in clinical practice resulting from the application of ART-SACC. Improvement Proportion Related to ART-SACC (IPR-ART-SACC) was calculated with the following formula:
IPR-ART-SACC=[number of times that ART-SACC changed clinical practice/(number of occasions that the SM was selected−number of occasions that the analysis of it did not proceed because the patient did not meet the inclusion criteria)]×100.
Feasibility was determined by the successful completion of auditing every day that it was attempted in order to evaluate whether it would be possible to include ART-SACC in daily care routines.
Statistical analysisData from the questionnaires were coded and entered into the Statistical Package for the Social Sciences (SPSS, version 15) database. Categorical variables were described by absolute and relative frequencies (%). For continuous variables, mean and standard deviation (SD) were used, or median and range if distribution was not normal.
ResultsTwenty-one experts were invited and agreed to participate in the study.
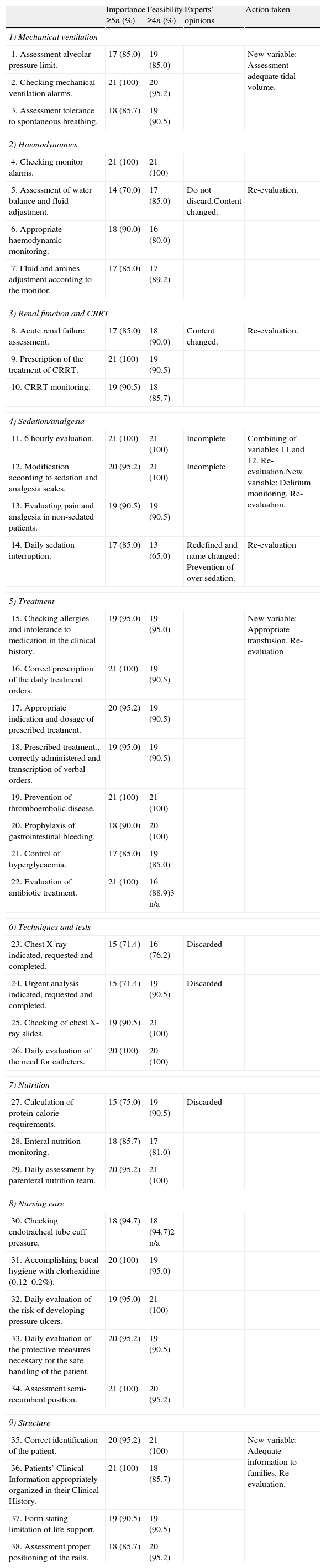
Delphi processTable 1 shows the initial list of SMs proposed by researchers. This table also summarizes the score in relation to importance and feasibility and the changes resulting from the intervention of experts in the three rounds of the process. No variables were removed due to polarization. Most changes were made in the area of Haemodynamics, Renal Function/CRRT and Sedation/Analgesia. In order to achieve a similar number of items in all areas block 5 (Treatment) was split into two.
List of SMs proposed by the research team and a summary of the modifications made over the 3 rounds of the Delphi process. CRRT (Continuous Renal Replacement Therapy).
| Importance ≥5n (%) | Feasibility ≥4n (%) | Experts’ opinions | Action taken | |
| 1) Mechanical ventilation | ||||
| 1. Assessment alveolar pressure limit. | 17 (85.0) | 19 (85.0) | New variable: Assessment adequate tidal volume. | |
| 2. Checking mechanical ventilation alarms. | 21 (100) | 20 (95.2) | ||
| 3. Assessment tolerance to spontaneous breathing. | 18 (85.7) | 19 (90.5) | ||
| 2) Haemodynamics | ||||
| 4. Checking monitor alarms. | 21 (100) | 21 (100) | ||
| 5. Assessment of water balance and fluid adjustment. | 14 (70.0) | 17 (85.0) | Do not discard.Content changed. | Re-evaluation. |
| 6. Appropriate haemodynamic monitoring. | 18 (90.0) | 16 (80.0) | ||
| 7. Fluid and amines adjustment according to the monitor. | 17 (85.0) | 17 (89.2) | ||
| 3) Renal function and CRRT | ||||
| 8. Acute renal failure assessment. | 17 (85.0) | 18 (90.0) | Content changed. | Re-evaluation. |
| 9. Prescription of the treatment of CRRT. | 21 (100) | 19 (90.5) | ||
| 10. CRRT monitoring. | 19 (90.5) | 18 (85.7) | ||
| 4) Sedation/analgesia | ||||
| 11. 6 hourly evaluation. | 21 (100) | 21 (100) | Incomplete | Combining of variables 11 and 12. Re-evaluation.New variable: Delirium monitoring. Re-evaluation. |
| 12. Modification according to sedation and analgesia scales. | 20 (95.2) | 21 (100) | Incomplete | |
| 13. Evaluating pain and analgesia in non-sedated patients. | 19 (90.5) | 19 (90.5) | ||
| 14. Daily sedation interruption. | 17 (85.0) | 13 (65.0) | Redefined and name changed: Prevention of over sedation. | Re-evaluation |
| 5) Treatment | ||||
| 15. Checking allergies and intolerance to medication in the clinical history. | 19 (95.0) | 19 (95.0) | New variable: Appropriate transfusion. Re-evaluation | |
| 16. Correct prescription of the daily treatment orders. | 21 (100) | 19 (90.5) | ||
| 17. Appropriate indication and dosage of prescribed treatment. | 20 (95.2) | 19 (90.5) | ||
| 18. Prescribed treatment., correctly administered and transcription of verbal orders. | 19 (95.0) | 19 (90.5) | ||
| 19. Prevention of thromboembolic disease. | 21 (100) | 21 (100) | ||
| 20. Prophylaxis of gastrointestinal bleeding. | 18 (90.0) | 20 (100) | ||
| 21. Control of hyperglycaemia. | 17 (85.0) | 19 (85.0) | ||
| 22. Evaluation of antibiotic treatment. | 21 (100) | 16 (88.9)3 n/a | ||
| 6) Techniques and tests | ||||
| 23. Chest X-ray indicated, requested and completed. | 15 (71.4) | 16 (76.2) | Discarded | |
| 24. Urgent analysis indicated, requested and completed. | 15 (71.4) | 19 (90.5) | Discarded | |
| 25. Checking of chest X-ray slides. | 19 (90.5) | 21 (100) | ||
| 26. Daily evaluation of the need for catheters. | 20 (100) | 20 (100) | ||
| 7) Nutrition | ||||
| 27. Calculation of protein-calorie requirements. | 15 (75.0) | 19 (90.5) | Discarded | |
| 28. Enteral nutrition monitoring. | 18 (85.7) | 17 (81.0) | ||
| 29. Daily assessment by parenteral nutrition team. | 20 (95.2) | 21 (100) | ||
| 8) Nursing care | ||||
| 30. Checking endotracheal tube cuff pressure. | 18 (94.7) | 18 (94.7)2 n/a | ||
| 31. Accomplishing bucal hygiene with clorhexidine (0.12–0.2%). | 20 (100) | 19 (95.0) | ||
| 32. Daily evaluation of the risk of developing pressure ulcers. | 19 (95.0) | 21 (100) | ||
| 33. Daily evaluation of the protective measures necessary for the safe handling of the patient. | 20 (95.2) | 19 (90.5) | ||
| 34. Assessment semi-recumbent position. | 21 (100) | 20 (95.2) | ||
| 9) Structure | ||||
| 35. Correct identification of the patient. | 20 (95.2) | 21 (100) | New variable: Adequate information to families. Re-evaluation. | |
| 36. Patients’ Clinical Information appropriately organized in their Clinical History. | 21 (100) | 18 (85.7) | ||
| 37. Form stating limitation of life-support. | 19 (90.5) | 19 (90.5) | ||
| 38. Assessment proper positioning of the rails. | 18 (85.7) | 20 (95.2) | ||
During the 14-day study period eighty-seven patients were evaluated. The mean of occupancy rate of was 96.7% (SD: 0.08). The mean of SOFA was 4.7 (SD 2.9) and of the length of stay was 10 days (range: 1–80). Admission diagnostic category was: 38 (43.7%) medical, 25 (28.7%) surgical, 20 (23%) neurocritical and 4 (4.6%) traumatic patients.
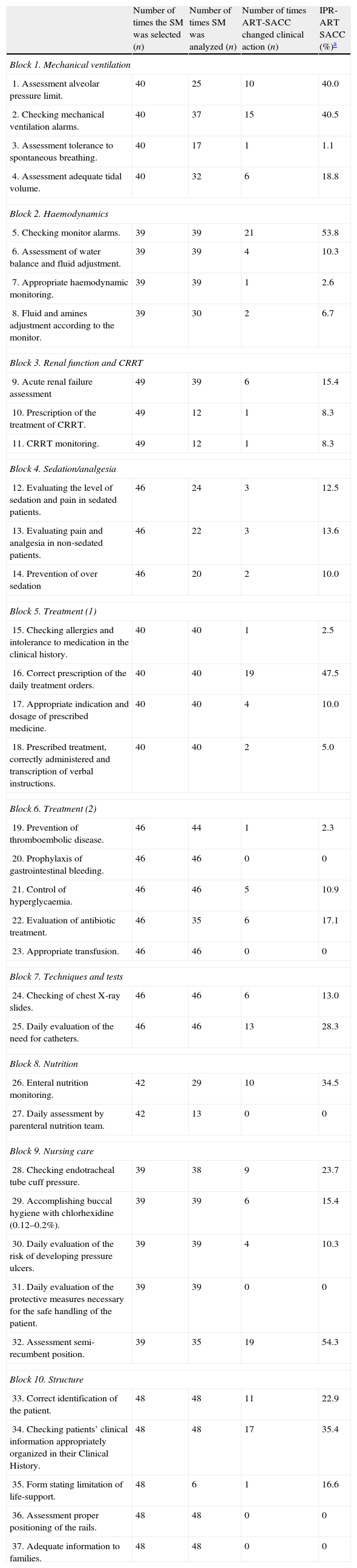
Utility and feasibility of ART-SACCUtility: Table 2 shows the final list of 37 SMs and the results of ART-SACC during the pilot study. In 31 of the 37 SMs (83.78%) analyzed, ART-SACC led to changes in clinical practice. By contrast, ART-SACC identified 6 SMs with no effect on changing the patient care because they had all been previously successful implemented. These six were as follows: prophylaxis of gastrointestinal bleeding, appropriate transfusion, daily assessment by parenteral nutrition team, daily evaluation of protective measures for the safe handling of the patient, assessment proper positioning of the rails, and adequate information to families.
Final list of SMs. Results of the ART-SACC pilot study. SM: safety measures. IPR-ART SACC: Improvement Proportion Related to ART-SACC. CRRT (Continuous Renal Replacement Therapy). Number of times SM was analyzed.
| Number of times the SM was selected (n) | Number of times SM was analyzed (n) | Number of times ART-SACC changed clinical action (n) | IPR-ART SACC (%)a | |
| Block 1. Mechanical ventilation | ||||
| 1. Assessment alveolar pressure limit. | 40 | 25 | 10 | 40.0 |
| 2. Checking mechanical ventilation alarms. | 40 | 37 | 15 | 40.5 |
| 3. Assessment tolerance to spontaneous breathing. | 40 | 17 | 1 | 1.1 |
| 4. Assessment adequate tidal volume. | 40 | 32 | 6 | 18.8 |
| Block 2. Haemodynamics | ||||
| 5. Checking monitor alarms. | 39 | 39 | 21 | 53.8 |
| 6. Assessment of water balance and fluid adjustment. | 39 | 39 | 4 | 10.3 |
| 7. Appropriate haemodynamic monitoring. | 39 | 39 | 1 | 2.6 |
| 8. Fluid and amines adjustment according to the monitor. | 39 | 30 | 2 | 6.7 |
| Block 3. Renal function and CRRT | ||||
| 9. Acute renal failure assessment | 49 | 39 | 6 | 15.4 |
| 10. Prescription of the treatment of CRRT. | 49 | 12 | 1 | 8.3 |
| 11. CRRT monitoring. | 49 | 12 | 1 | 8.3 |
| Block 4. Sedation/analgesia | ||||
| 12. Evaluating the level of sedation and pain in sedated patients. | 46 | 24 | 3 | 12.5 |
| 13. Evaluating pain and analgesia in non-sedated patients. | 46 | 22 | 3 | 13.6 |
| 14. Prevention of over sedation | 46 | 20 | 2 | 10.0 |
| Block 5. Treatment (1) | ||||
| 15. Checking allergies and intolerance to medication in the clinical history. | 40 | 40 | 1 | 2.5 |
| 16. Correct prescription of the daily treatment orders. | 40 | 40 | 19 | 47.5 |
| 17. Appropriate indication and dosage of prescribed medicine. | 40 | 40 | 4 | 10.0 |
| 18. Prescribed treatment, correctly administered and transcription of verbal instructions. | 40 | 40 | 2 | 5.0 |
| Block 6. Treatment (2) | ||||
| 19. Prevention of thromboembolic disease. | 46 | 44 | 1 | 2.3 |
| 20. Prophylaxis of gastrointestinal bleeding. | 46 | 46 | 0 | 0 |
| 21. Control of hyperglycaemia. | 46 | 46 | 5 | 10.9 |
| 22. Evaluation of antibiotic treatment. | 46 | 35 | 6 | 17.1 |
| 23. Appropriate transfusion. | 46 | 46 | 0 | 0 |
| Block 7. Techniques and tests | ||||
| 24. Checking of chest X-ray slides. | 46 | 46 | 6 | 13.0 |
| 25. Daily evaluation of the need for catheters. | 46 | 46 | 13 | 28.3 |
| Block 8. Nutrition | ||||
| 26. Enteral nutrition monitoring. | 42 | 29 | 10 | 34.5 |
| 27. Daily assessment by parenteral nutrition team. | 42 | 13 | 0 | 0 |
| Block 9. Nursing care | ||||
| 28. Checking endotracheal tube cuff pressure. | 39 | 38 | 9 | 23.7 |
| 29. Accomplishing buccal hygiene with chlorhexidine (0.12–0.2%). | 39 | 39 | 6 | 15.4 |
| 30. Daily evaluation of the risk of developing pressure ulcers. | 39 | 39 | 4 | 10.3 |
| 31. Daily evaluation of the protective measures necessary for the safe handling of the patient. | 39 | 39 | 0 | 0 |
| 32. Assessment semi-recumbent position. | 39 | 35 | 19 | 54.3 |
| Block 10. Structure | ||||
| 33. Correct identification of the patient. | 48 | 48 | 11 | 22.9 |
| 34. Checking patients’ clinical information appropriately organized in their Clinical History. | 48 | 48 | 17 | 35.4 |
| 35. Form stating limitation of life-support. | 48 | 6 | 1 | 16.6 |
| 36. Assessment proper positioning of the rails. | 48 | 48 | 0 | 0 |
| 37. Adequate information to families. | 48 | 48 | 0 | 0 |
Notably, there were SMs for which the IPR-ART-SACC was over 25%. These were as follows: assessment of the alveolar pressure limit, checking mechanical ventilation alarms, checking monitor alarms, correct prescription of the daily treatment orders, daily evaluation of the need for catheters, enteral nutrition monitoring, assessment of semi-recumbent position, and checking patients’ clinical information appropriately organized in their Clinical History.
The answer “No”, which implies the impossibility of changing clinical performance, was recorded in these two variables: control of hyperglycaemia and prescribed treatment, correctly administered including transcription of verbal orders (in 7 and 6 cases, respectively).
Feasibility: In this pilot study, ART-SACC audits were carried out on all of the scheduled days. Clinical priorities (such as urgent techniques, urgent transfer to surgery or radiology room) delayed 20% of the evaluations.
DiscussionDespite the awareness of patient safety and quality of care issues increasing in both clinical and political arenas, the translation into research and clinical practice has been incomplete although the topic has been found to have significant benefits.26 To our knowledge, this is the first study designed to build a clinically useful tool aimed at improving the care and safety of critical adult patients with the following characteristics: aimed to prevent errors of omission and commission, easily applied by the clinician during routine clinical work, and finally, rendering useful information that can be applied immediately by modifying the care regimen of the critical patient. This study has been conducted within the context of an effort of our institution and our ICU to gradually establish a culture of non-punitive safety at conjunctural moment aimed at reshaping medical practice.27
The Delphi method, used to achieve consensus among experts, has been useful in defining the SMs contained in the checklist. Significant qualitative modifications were made in some cases. In particular, the content of the SMs “Assessing water balance and fluid adjustment” and “Acute renal failure assessment” were modified sequentially in all three rounds of Delphi, which shows the effort it takes to reach consensus on controversial issues in the management of critically ill patients. On the other hand, consensus was simple in aspects that are included in national or international guidelines.28
Ursprung et al.17 conducted an interesting pilot study in a neonatal intensive care unit looking at the feasibility and utility of a real-time safety auditing programme that takes place during routine clinical work. The authors showed that real-time safety audits can flag up a broad range of errors. Their study design, however, did not allow errors of omission that might occur in important areas of critical patient management. In this current pilot study, the detection of errors of omission was paramount. For example, ART-SACC has promoted daily reflection on important aspects of critical care, such as fluid adjustment or antibiotic treatment, since it is well known that an adequate or appropriate balance of fluids and/or an adequate antibiotic treatment impacts on the prognosis of critical patients.29,30 In that way, this pilot study suggests the utility of ART-SACC for promoting changes in patient care using a tool designed to limit errors of omission and commission.
Other authors31 have also conducted random safety studies in neonatal ICUs, although focussing their analysis exclusively on issues related to infection. This approach may not be sufficient in the context of the complexity of critical patients. ART-SACC was designed as a functional tool to assist the clinician in the structuring of essential clinical decisions such as assessing haemodynamics, renal failure, sedoanalgesia and nutrition, in addition to infection. In another study, Simpson et al.32 tried to assess the impact of a checklist of clinical safety in critical patient care. They concluded that they were unable to measure, with certainty, the exact impact that the checklist had on discovering errors and omissions in ICU care. In order to address this issue, in the present study a variable aimed to quantify the impact of daily random evaluations was created: “Improvement Proportion Related to ART-SACC (IPR-ART-SACC)”.
It is important to highlight that those SMs clearly defined by international guidelines had a high IPR-ART-SACC. For example, the “assessing adequate tidal volume” had an IPR-ART-SACC of 18.8%. Of particular concern are SMs whose IPR-ART-SACC was over 25%. SMs with a high IPR-ART-SACC require specific analysis in order to plan strategies that will improve the quality of care. It would be expected that, following the implementation of improvement plans, the IPR-ART-SACC would progressively decrease. In this way, ART-SACC could be considered a tool for monitoring the impact of actions (protocols, clinical guidelines, training, etc.) in clinical processes that require improvement.
The “No” answers are also relevant because they did not allow any instant changes in clinical approach. However, the SMs to which there was a “No” response, such as the glycaemia control protocol and the verbal orders policies had been recently addressed as part of the routine clinical in our ICU and considered for urgent completion in specific protocol recently implemented in our ICU.
It was not a specific objective in this study to evaluate how acceptable ART-SACC would be in our ICU, but the clinicians who were involved were generally responsive and helpful. Unlike the experience reported by Ursprung et al.,17 our research team did not receive any comments about reducing the number of SMs in each assessment. Perhaps the randomness of patients and SMs served to improve collaboration and maintain alertness in the healthcare staff, something that we consider beneficial in places such as the ICU, which handles a large amount of information. Furthermore, in some ways, doing it this way reduces the impact of possible bias associated to any observation. Undoubtedly, another aspect that has helped staff to accept ART-SACC has been the absence of punitive consequences. On the contrary, the exchange of views held at bedside has been instructive in many cases from the educational point of view.
This pilot study has had several limitations. Firstly, there were a small number of audits. Secondly, the SMs included in ART-SACC were designed and adjusted to the needs of a single centre. In future studies, in order to attain external validity, will be important to include other ICUs with different levels of complexity. Thirdly, although the information extracted and the perception of the study was positive, the time spent performing ART-SACC needs to be evaluated because it is a variable that is directly related to its feasibility, particularly if it is considered in the mid and long term. Finally, it probably would have been helpful to know the incidence of errors of commission and omission before and after the study.
In conclusion, the Delphi method was useful for designing and compiling the list of 37 SMs that were scheduled in 10 blocks. The utility of ART-SACC was assessed through the IPR-ART-SACC. The audits helped to direct attention towards minimizing errors (action or omission) and improving clinical care in more than 85% of the selected SMs. Although feasibility was adequate and acceptance seems positive, the quantification of the resources used, essentially time spent on developing ART-SACC, has to be considered if this tool is to be implemented in routine clinical work and more centres with different levels of complexity are to be involved.
ContributorsSirgo G, Olona M, Martin MC, Esteban F, Pobo A and Bodí M have made substantial contributions to conception and design, acquisition, analysis and interpretation of data. Sirgo G has drafted the submitted article. Olona M, Martin MC, Esteban F, Pobo A and Bodí M, have revised the manuscript critically for important intellectual content. ART-SACC study Experts: Alonso A, Benito E, Cabré Ll, Calvo E, Chamorro C, Corral E, De Mendoza D, Diaz E, Grau S, Gutiérrez I, León C, Maynar J, Merino P, Ochagavía A, Quesada A, Alba A, Roca J, Rodríguez A, Sagrera C, Sirvent JM, Vallés J have made substantial contributions to conception and design during the Delphi process and have revised the manuscript critically for important intellectual content.
FundingThis study was supported by grants from the Fondo de Investigación Sanitaria (ISCIII, FIS grants, project PI11/02311). The funding agency had no role in study design, in collection, analysis or interpretation of data; in writing of the manuscript; or in the decision to submit the paper for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Institute of Health Carlos III (ISC III) from Spain.
Conflict of interestThe authors have no conflict of interest to disclose.
ART-SACC study experts are listed in Appendix A.

