

Both treatment and prevention of infections are an essential part of the daily routine of Intensive Care Units (ICU, assigned to Intensive Care Medicine Service) and Reanimation Units (RU, assigned to Anesthesia and Reanimation Service)
The incidence of sepsis on admission or during the stay in these units is high 1 so,1 this experience has made intensivists play an important role in the development of Sepsis Code (SC).2–4
In the field of prevention of healthcare-related infections (HCRI), the Program for Safety in the Critically Ill Patient has been developed by the Spanish Society of Intensive Care Medicine (SEMICYUC), which consists of preparing and implementing the Zero Projects (ZP): Zero Bacteremia (ZB), Zero Pneumonia, Zero Resistanceand Zero Urinary Tract Infection (Z-UTI).5
Antimicrobial Stewardship Programs (ASP),6,7 with the aim of improving the clinical outcome of infected patients and minimizing adverse effects of antibiotics (including appearance and spread of antimicrobial resistance), have a wide margin of action in critical care units, both as part of hospital ASP or as specific ICUs programs.8,9
In order to measure the degree of implementation of SC, ZP and ASP, and the role played by intensivists/anesthesiologists, the main national study groups of infection in critically ill patient (GEIPC-SEIMC, GTEIS-SEMICYUC and GTIPO-SEDAR) designed an online questionnaire that was mailed (in January 2019) to all members of the aforementioned groups requesting the response of the department heads.
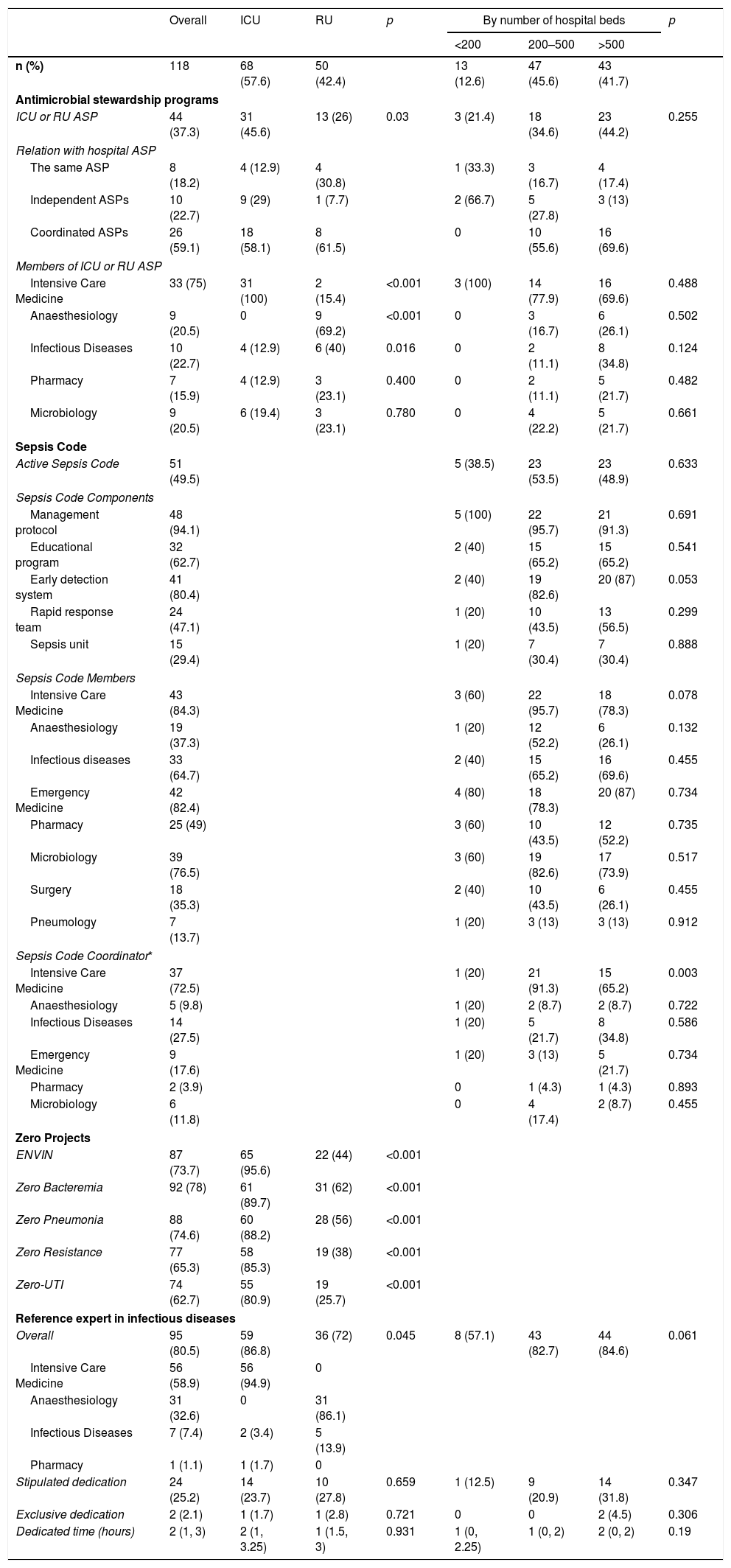
We received answers from 118 units and 103 hospitals. Table 1 summarizes our main findings. Qualitative variables were compared using Chi-square.
Main findings of our survey.
| Overall | ICU | RU | p | By number of hospital beds | p | |||
|---|---|---|---|---|---|---|---|---|
| <200 | 200–500 | >500 | ||||||
| n (%) | 118 | 68 (57.6) | 50 (42.4) | 13 (12.6) | 47 (45.6) | 43 (41.7) | ||
| Antimicrobial stewardship programs | ||||||||
| ICU or RU ASP | 44 (37.3) | 31 (45.6) | 13 (26) | 0.03 | 3 (21.4) | 18 (34.6) | 23 (44.2) | 0.255 |
| Relation with hospital ASP | ||||||||
| The same ASP | 8 (18.2) | 4 (12.9) | 4 (30.8) | 1 (33.3) | 3 (16.7) | 4 (17.4) | ||
| Independent ASPs | 10 (22.7) | 9 (29) | 1 (7.7) | 2 (66.7) | 5 (27.8) | 3 (13) | ||
| Coordinated ASPs | 26 (59.1) | 18 (58.1) | 8 (61.5) | 0 | 10 (55.6) | 16 (69.6) | ||
| Members of ICU or RU ASP | ||||||||
| Intensive Care Medicine | 33 (75) | 31 (100) | 2 (15.4) | <0.001 | 3 (100) | 14 (77.9) | 16 (69.6) | 0.488 |
| Anaesthesiology | 9 (20.5) | 0 | 9 (69.2) | <0.001 | 0 | 3 (16.7) | 6 (26.1) | 0.502 |
| Infectious Diseases | 10 (22.7) | 4 (12.9) | 6 (40) | 0.016 | 0 | 2 (11.1) | 8 (34.8) | 0.124 |
| Pharmacy | 7 (15.9) | 4 (12.9) | 3 (23.1) | 0.400 | 0 | 2 (11.1) | 5 (21.7) | 0.482 |
| Microbiology | 9 (20.5) | 6 (19.4) | 3 (23.1) | 0.780 | 0 | 4 (22.2) | 5 (21.7) | 0.661 |
| Sepsis Code | ||||||||
| Active Sepsis Code | 51 (49.5) | 5 (38.5) | 23 (53.5) | 23 (48.9) | 0.633 | |||
| Sepsis Code Components | ||||||||
| Management protocol | 48 (94.1) | 5 (100) | 22 (95.7) | 21 (91.3) | 0.691 | |||
| Educational program | 32 (62.7) | 2 (40) | 15 (65.2) | 15 (65.2) | 0.541 | |||
| Early detection system | 41 (80.4) | 2 (40) | 19 (82.6) | 20 (87) | 0.053 | |||
| Rapid response team | 24 (47.1) | 1 (20) | 10 (43.5) | 13 (56.5) | 0.299 | |||
| Sepsis unit | 15 (29.4) | 1 (20) | 7 (30.4) | 7 (30.4) | 0.888 | |||
| Sepsis Code Members | ||||||||
| Intensive Care Medicine | 43 (84.3) | 3 (60) | 22 (95.7) | 18 (78.3) | 0.078 | |||
| Anaesthesiology | 19 (37.3) | 1 (20) | 12 (52.2) | 6 (26.1) | 0.132 | |||
| Infectious diseases | 33 (64.7) | 2 (40) | 15 (65.2) | 16 (69.6) | 0.455 | |||
| Emergency Medicine | 42 (82.4) | 4 (80) | 18 (78.3) | 20 (87) | 0.734 | |||
| Pharmacy | 25 (49) | 3 (60) | 10 (43.5) | 12 (52.2) | 0.735 | |||
| Microbiology | 39 (76.5) | 3 (60) | 19 (82.6) | 17 (73.9) | 0.517 | |||
| Surgery | 18 (35.3) | 2 (40) | 10 (43.5) | 6 (26.1) | 0.455 | |||
| Pneumology | 7 (13.7) | 1 (20) | 3 (13) | 3 (13) | 0.912 | |||
| Sepsis Code Coordinator* | ||||||||
| Intensive Care Medicine | 37 (72.5) | 1 (20) | 21 (91.3) | 15 (65.2) | 0.003 | |||
| Anaesthesiology | 5 (9.8) | 1 (20) | 2 (8.7) | 2 (8.7) | 0.722 | |||
| Infectious Diseases | 14 (27.5) | 1 (20) | 5 (21.7) | 8 (34.8) | 0.586 | |||
| Emergency Medicine | 9 (17.6) | 1 (20) | 3 (13) | 5 (21.7) | 0.734 | |||
| Pharmacy | 2 (3.9) | 0 | 1 (4.3) | 1 (4.3) | 0.893 | |||
| Microbiology | 6 (11.8) | 0 | 4 (17.4) | 2 (8.7) | 0.455 | |||
| Zero Projects | ||||||||
| ENVIN | 87 (73.7) | 65 (95.6) | 22 (44) | <0.001 | ||||
| Zero Bacteremia | 92 (78) | 61 (89.7) | 31 (62) | <0.001 | ||||
| Zero Pneumonia | 88 (74.6) | 60 (88.2) | 28 (56) | <0.001 | ||||
| Zero Resistance | 77 (65.3) | 58 (85.3) | 19 (38) | <0.001 | ||||
| Zero-UTI | 74 (62.7) | 55 (80.9) | 19 (25.7) | <0.001 | ||||
| Reference expert in infectious diseases | ||||||||
| Overall | 95 (80.5) | 59 (86.8) | 36 (72) | 0.045 | 8 (57.1) | 43 (82.7) | 44 (84.6) | 0.061 |
| Intensive Care Medicine | 56 (58.9) | 56 (94.9) | 0 | |||||
| Anaesthesiology | 31 (32.6) | 0 | 31 (86.1) | |||||
| Infectious Diseases | 7 (7.4) | 2 (3.4) | 5 (13.9) | |||||
| Pharmacy | 1 (1.1) | 1 (1.7) | 0 | |||||
| Stipulated dedication | 24 (25.2) | 14 (23.7) | 10 (27.8) | 0.659 | 1 (12.5) | 9 (20.9) | 14 (31.8) | 0.347 |
| Exclusive dedication | 2 (2.1) | 1 (1.7) | 1 (2.8) | 0.721 | 0 | 0 | 2 (4.5) | 0.306 |
| Dedicated time (hours) | 2 (1, 3) | 2 (1, 3.25) | 1 (1.5, 3) | 0.931 | 1 (0, 2.25) | 1 (0, 2) | 2 (0, 2) | 0.19 |
We observed that ZP is implemented in most units, ranging from 62.7% for Zero-UTI (the latest program) to 78.0% for ZB. We must bear in mind that adherence is higher in ICUs (80.9% of ICUs have joined Zero-UTI and up to 89.7% take part in ZB; compared to RUs, in which only 25.7% have implanted Zero-UTI, increasing to 62% for ZB. 3 out of every 4 units uses the Spanish Study for Monitoring Nosocomial Infection (ENVIN, developed by SEMICYUC) as a monitoring tool for HCRI. Its use is widespread in ICUs (95.6%) and scarce in RUs (44%).
Less than half of hospitals have an active SC, 38.5% in the smallest. SC have several components: 94.1% of SC have a protocol; early detection systems are the next most commonly implemented component (80%), and only 29.4% SC have a team specifically focused on sepsis management. The role of intensivists in SC is remarkable: they are only absent in 15.7 and coordinate 72.5%. Also notable is the role of Emergency Medicine physicians, who are present in 82.4% of teams and especially important in the smallest hospitals.
Only 37.3% of units have an ASP, being more common in large hospitals. In general, the ICU-RU ASP works in a coordination with the hospital ASP although it is notable that 29% of ICU-ASPs are independent. At least one intensivist participates in all ICU-ASPs, supported essentially by the Microbiology Department. The composition of RU-ASP is heterogeneous with the participation of specialists from Infectious Diseases (ID), Pharmacy and Microbiology units, in addition to anesthesiologists themselves.
It is noteworthy that 80.5% of units have a reference expert in infectious diseases; more frequent in ICUs (86.8%) than in RUs (72.0%) (p=0.045) and, often, a specialist from the unit itself (94.9% of ICUs and 86.1% of RUs). Despite the workload of these programs, only 25.2% of reference experts have a reserved daily work time dedicated to these programs.
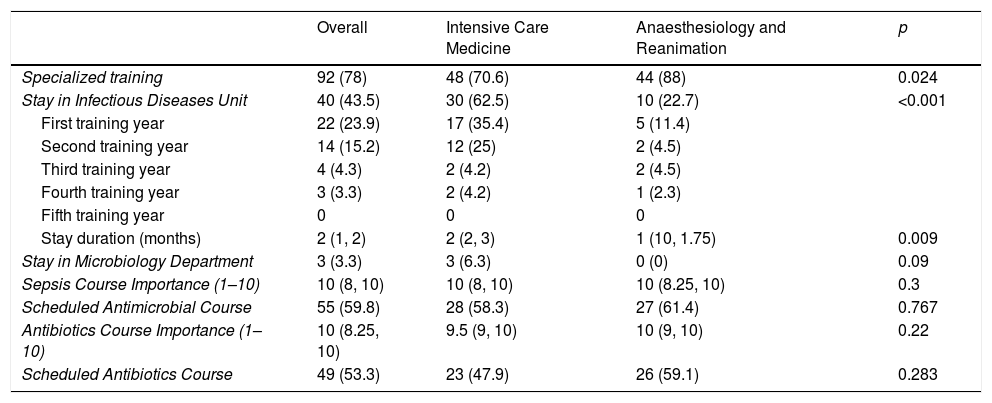
A high percentage of units taking part in our study train residents in Intensive Care Medicine (ICM) or Anesthesiology (Table 2). Less than half of residents have a scheduled stay in an ID unit, being more common among ICM residents (62.5% vs 22.7%, p<0.001). Stays in the Microbiology Department are anecdotal. We have observed a significant discrepancy between the importance attributed to sepsis and antibiotic courses (according to the perception of the person who answers the survey) and the number of residents who have these courses scheduled.
Scheduled training in infectious diseases during the training period.
| Overall | Intensive Care Medicine | Anaesthesiology and Reanimation | p | |
|---|---|---|---|---|
| Specialized training | 92 (78) | 48 (70.6) | 44 (88) | 0.024 |
| Stay in Infectious Diseases Unit | 40 (43.5) | 30 (62.5) | 10 (22.7) | <0.001 |
| First training year | 22 (23.9) | 17 (35.4) | 5 (11.4) | |
| Second training year | 14 (15.2) | 12 (25) | 2 (4.5) | |
| Third training year | 4 (4.3) | 2 (4.2) | 2 (4.5) | |
| Fourth training year | 3 (3.3) | 2 (4.2) | 1 (2.3) | |
| Fifth training year | 0 | 0 | 0 | |
| Stay duration (months) | 2 (1, 2) | 2 (2, 3) | 1 (10, 1.75) | 0.009 |
| Stay in Microbiology Department | 3 (3.3) | 3 (6.3) | 0 (0) | 0.09 |
| Sepsis Course Importance (1–10) | 10 (8, 10) | 10 (8, 10) | 10 (8.25, 10) | 0.3 |
| Scheduled Antimicrobial Course | 55 (59.8) | 28 (58.3) | 27 (61.4) | 0.767 |
| Antibiotics Course Importance (1–10) | 10 (8.25, 10) | 9.5 (9, 10) | 10 (9, 10) | 0.22 |
| Scheduled Antibiotics Course | 49 (53.3) | 23 (47.9) | 26 (59.1) | 0.283 |
Our study has detected important differences between ICUs and RUs. First, adherence to ZP is significantly higher in ICUs than in RUs. Secondly, the number of ICUs in which an ASP has been implanted is significantly higher than RUs. Thirdly, the participation of intensivists in SC is greater; leading most of the active SCs in Spain. Finally, ICM resident training programs place greater importance to infectious diseases, with a greater number and longer stays in ID units.
The data provided by this study may be of interest to design strategies from scientific societies or autonomous communities, aimed at increasing the implantation of these programs. Given that HCRI prevention programs are broadly implanted, in our opinion, efforts should be directed at creating ASPs and SC, especially in hospitals with less than 200 beds (only 38.5% have a Sepsis Code and 21.4% an ASP for critically ill patients). Those units with more developed programs may serve as a model for others interested in developing them.
Another point for improvement detected is the lack of specific training in infectious diseases of residents in ICM and especially, Anesthesiology.
One of the limitations of this study is that participation was voluntary, and it is possible that just the units most interested in these programs have participated. Despite this, a good number of units took part and almost all Spanish Autonomous Communities were represented (16 of 17). The degree of real adherence to each project was not evaluated either.
From our results it could be inferred that, despite the existence of several programs related to infectious pathology in the critically ill patient (as SC, ZP and ASP), in ICUs and RUs of our environment, there are no structures or specialists with enough dedication to implant them optimally, follow them and coordinate them. We could hypothesize that initiatives such as SEMICYUC accreditation of experts in infectious pathology in the critically ill patient, together with allocation of specific resources to these programs (especially working time for specialists who lead them) would increase the number and quality of active programs.
We want to record our appreciation to the 118 colleagues who have answered the questionnaire and participated in this survey.
The authors thank the Illustrious Medical College of Ourense for their collaboration in the English translation of this article.

