








Edited by: Federico Gordo. Intensive Care Service of Hospital of Henares, Madrid, Spain
Last update: April 2025
More infoThe human condition is linked to error in any activity that is performed, and the healthcare world is no exception. The origin of human error does not lie within the perversity of human nature, instead, it has its origins in latent failures in the healthcare environment and is a consequence of the processes and procedures applied. The science of the Human Factor deals with the application of knowledge to people (capabilities, characteristics and limitations), with the design and the management of the equipment they use and with the environments in which they work and the activities they carry out.
Part of the Human Factor are the non-technical skills. These skills greatly influence people's behavior and, therefore, their performance and the quality of healthcare in a very complex socio-technical system.
La condición humana esta&#¿; ligada al error en cualquier actividad y el mundo sanitario no es la excepción. Los errores humanos, esperables o previsibles, no tienen su origen en la perversidad de la naturaleza humana, sino en fallos latentes en el entorno asistencial y son consecuencia de los procesos y procedimientos que se aplican. En este sentido, surge la ciencia del Factor Humano que se ocupa de la aplicación del conocimiento sobre las personas (capacidades, características y limitaciones), diseño y gestión de los equipos que utilizan, entornos en los que trabajan y las actividades que tienen que realizar en el marco de un sistema socio-técnico muy complejo como es el mundo sanitario.
Dentro del extenso campo que engloba los Factores Humanos, las características humanas e individuales influyen enormemente sobre el comportamiento de las personas y, por tanto, en su rendimiento y calidad de la atención sanitaria.
The human condition is linked to error in any kind of activity performed, and the healthcare setting is no exception to this. Indeed, in healthcare, perfection expectations are neither realistic nor possible. In this respect, Patient Safety plays a key role not in eliminating human errors but in understanding why they occur, reducing avoidable errors and preventing undesired harm.
These human errors, avoidable or foreseeable, do not originate from the perversity of human nature but rather comprise latent defects in the healthcare environment and are a consequence of the processes and procedures applied. The science of the Human Factor (HF) emerges in this respect as the application of knowledge about people (capacities, characteristics and limitations), the design and management of the equipment used, the working environments involved, and the activities carried out in a highly complex socio-technical system like the world of healthcare.1 The application of the HF helps reduce the risk of incidents, and when incidents do occur, it contributes to allowing healthcare professionals to respond correctly.2,3 In other words, the FH seeks to secure an adequate performance of both the professionals and the system, but also adopts an approach intended to optimize worker wellbeing.
The present study explores the general definitions and concepts involved, and describes the types of human skills and tools for training and/or implementing them.
Definition of “Human Factor” and “Ergonomics”The term “Human Factor” is sometimes confusing. When people not familiar with this terminology hear that an accident has been due to a Human Factor, they often understand that the accident has occurred because a “human at fault” made a mistake. Far from this perception, the science of the Human Factor rejects a person or group of people as being completely responsible for errors that occur in the context of a very complex socio-technical system.1 Experts in Human Factor see people as just another piece within the immense and complex puzzle represented by healthcare systems.
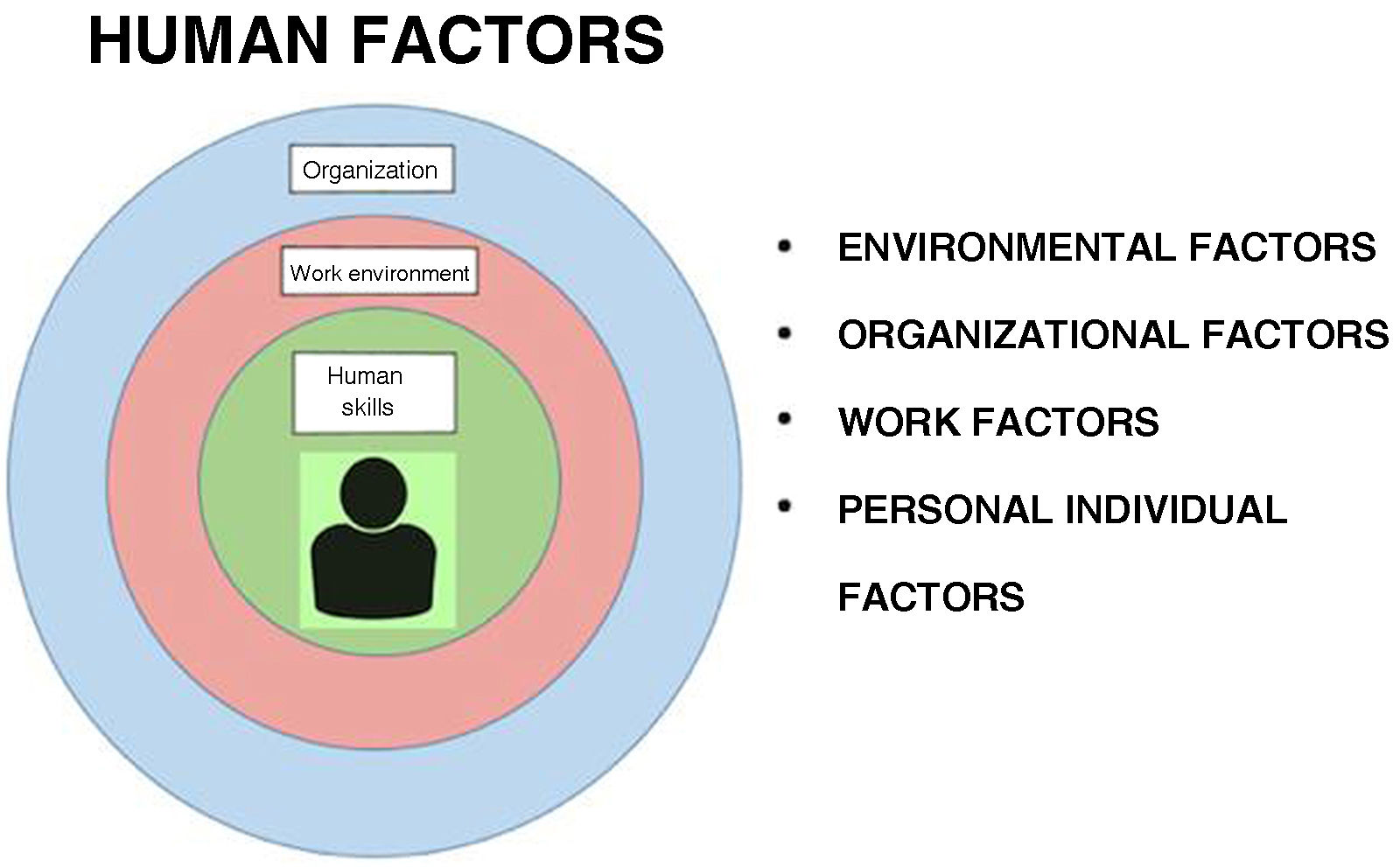
The term “Human Factor” has been defined in different ways. One of the most widely accepted definitions is that made by the industrial safety regulating body of the United Kingdom2: “Human Factors refer to environmental, organizational and work factors, and also to human and individual characteristics that influence the behavior of people in the workplace, with a potential impact upon health and safety. A simple way to view Human Factors is to think of three levels: the work, the person, and the organization, and to then examine how these aspects influence the behaviors of individuals in relation to health and safety” (Fig. 1).
An element closely related to the Human Factor is ergonomics, which consists on applying scientific information referred to the design of objects, systems and surroundings for human use,3 i.e., ergonomics involves the designing of workplaces, tools and tasks to make them coincide with the physiological, anatomical, psychological characteristics and capacities of the workers involved. In practice, the terms “Human Factor” and “ergonomics” are used as synonyms that seek to describe the relationships among people in their work, the activity they perform, and the working environment in itself.4
Although Patient Safety and the Human Factor are increasingly known concepts, in a world where the complexity of healthcare organisms and health processes is constantly increasing, it is important for healthcare professionals to be familiarized with the basic aspects of the science of the Human Factor and to identify how this discipline impacts upon daily work. The published evidence indicates that human errors, understood as deficiencies within the broad concept of the Human Factor, are responsible for between 80 and 90% of all adverse events that occur in healthcare institutions.5
The science of the Human Factor encompasses the study of technological as well as social problems. Understanding work as it is done in real life makes it possible to develop systems supporting the performance of such work, reducing the appearance of errors, improving working conditions, and increasing labor efficiency and satisfaction. This approach seeks to develop safer, more efficient and resilient work systems. To reach these objectives, the science of the Human Factor applies methods that come from engineering, psychology, biomechanics and the social sciences. For example, based on data referred to body size and biomechanics, it is possible to design computer workstations that reduce the risk of injury caused by repetitive efforts, or devices that can help lift patients and avoid injuries to healthcare staff. Furthermore, based on perceptive and cognitive characteristics (such as memory and attention), it is possible to design adequate interfaces to ensure good interaction between people and the electronic devices used in healthcare: screens and controls that are easy to understand and user-friendly.4
Lastly, it is important to note that when speaking of Human Factors, we almost always center our attention on errors, with the aim of understanding and minimizing them. However, the science of the Human Factor can also be applied to understand why things are working well, in order to identify those aspects that function correctly and export them to other areas.
Human skillsWithin the wide field of Human Factors, the individual characteristics of people largely influence their behavior, and therefore their performance and the quality of healthcare. When considering the critically ill patient, we could think that the Human Factor focuses mainly on everything surrounding the patient at the organizational and environmental level, where technology sometimes predominates. However, in critically ill patients, a very important intervening factor is represented by the human skills of the professionals who care for them, and which complement the traditional training received by the majority of healthcare professionals, based on the acquisition of knowledge and the mastering of technical skills such as airway management, the catheter placement, etc.3
Human skills can be defined as those cognitive and social capabilities that complement technical skills and contribute to safe and efficient task performance. One of the leading persons in this field is professor Rhona Flinn,6 who in her book Safety at the Sharp End highlighted 6 fundamental human skills as being most often implicated in adverse events: decision-making, communication, teamwork and leadership, situational awareness and the management of stress and fatigue6 (Table 1).
Human skills.6
| Cognitive: Situation awareness and decision-making |
| Social: Communication, teamwork and leadership |
| Personal limitations: Management of stress and fatigue |
This particular skill refers to the capacity to recognize and comprehensively understand our surroundings, but also to the identification and evaluation of the possible existing risks based on the information received from multiple sources, to anticipate future events. Three phases can be distinguished7:
- 1
Perception of the surrounding elements: this refers to adequately obtaining relevant information despite difficult conditions (environmental noise, poor illumination, etc.).
- 2
Understanding: this involves the integration, interpretation and adequate comprehension of the information received. In other words, it implies the capacity of people to develop a mental model that makes sense of the available information.
- 3
Prediction or projection: based on the information received and interpreted, people must be able to anticipate the appearance of future events and adopt measures to deal with them.
Decision-making refers to the capacity of people to judge or choose the best option suited to the needs of assessed or foreseen events, as well as unforeseen events, based on the multiple options that characterize a situation. In general, decisions are made by people after a prior evaluation of the situation, with the identification of the problem, the establishment of a diagnosis, and the evaluation of risks. Once the decision has been made and applied, it is advisable to re-evaluate the patient's response to the decision.8
CommunicationCommunication is a crucial skill that serves as a vehicle for transmitting information and constructing a common world with shared mental models. Although communication is encompassed within social skills, it is not just another human skill. Indeed, communication is the most important skill, since it serves as a binding link with the rest of human skills and a structuring element of human actions.9 Furthermore, in daily clinical practice, when caring for patients in a medical or surgical emergency, deficient communication between healthcare professionals may occur, and such ineffective communication in turn is the root cause of 60–80 % of all adverse effects and sentinel events.5,10 The main causes of these team communication problems are essentially related to the lack of use of a specific methodology, or shortcomings in professional training.11 In order to minimize these problems, healthcare professionals must seek to establish effective communication, defined as that which allows the exchanging of messages in such a way that the perception of the receiving person is identical to that of the person emitting the message. In other words, the aim is to generate a mental model shared among the different intervening individuals. This objective must be met when the healthcare professionals interact and transfer information to other people (whether patients or their families), or when they speak with other healthcare professionals.3,8
Although some people possess innate communication skills referred to as both verbal and non-verbal language, such skills - in the same way as with all skills - require training from the start, with the search for improvement based on standardized communication techniques.11,12 In this respect, closed-loop communication processes are essential,13 in the same way as structured communication techniques such as “SBAR” (Situation-Background-Assessment- Recommendation)14 or its variants (e.g., “ISBAR” [Identify-Situation-Background- Assessment-Recommendation] and “iSoBAR” (identify-Situation-observations-Background-Agreed plan-Read back]).15 Regarding closed-loop communication, in stressing and high-complexity situations this strategy allows the professionals (issuers and receivers) belonging to the team to check that the message has been correctly understood, guaranteeing that all the team members exchange information in a clear, concise and unambiguous manner.13 With regard to SBAR, this verbal or written communication tool is easy to use and very useful for the healthcare team members for exchanging essential and concise patient information (e.g., nurse to nurse, nurse to physician or physician to physician), reducing the need for repetition and the risk of mistakes in situations of crisis.14
On the other hand, healthcare professionals must be able to give “bad news” to patients and/or their families – a difficult task that requires professionalism, patience and training. The different training programs available for this purpose include multiple structured tools. One of the best-known is SPIKES (Strategy, Perception, Invitation, Knowledge, Empathy, Summary).16,17 SPIKES is a communication tool focused on the patient that includes a structured listening format that globally proposes the following: gathering all the information available on the patient and his or her situation; providing understandable information adjusted to the needs and desires; reducing the emotional impact which bad news has upon the receptor; and including the person in the intervention plan (Table 217).
Buckman protocol.16
| 1. Prepare the adequate physical context |
| 2. Investigate what the person knows |
| 3. Explore what the person wants to know |
| 4. Share the corresponding information |
| 5. Respond to feelings with empathy |
| 6. Planning and follow-up |
Critical situations in general are complex events that cannot be resolved by a single or by various people sequentially. Scenarios of this kind require the simultaneous participation of different professionals as a team to solve the problem.
A team is defined as two or more individuals that work together to reach a common series of goals, with specific competencies and specialized work roles, using shared resources and communicating together to coordinate.18 This definition includes two key elements within the work as a team. Firstly, ultimate success depends not only on the intervention of the individual as a member of the team but also on the skill of all its components to operate in a coordinated and effective way. This means that each professional must have general teamwork competencies or skills. Secondly, teamwork is closely linked to other human skills. In high-stress situations, such as a life-threatening emergencies, adequate leadership and effective communication among the different team members are crucial to ensure that a group of healthcare professionals can work together in an optimal way.19–22 This distinguishes a team consisting of a group of experts from a high-performance expert team.23
LeadershipThe team must have a person acting as the orchestra director, with a well-defined role: Leadership. Leadership is the series of management or directive skills that an individual has for influencing the behavior of a certain person or group of persons, causing this team to work with enthusiasm, giving the best of themselves to obtain a desired result. This implies the development and communication of a futuristc view, motivating people and securing their commitment.24 Leaders must have multiple qualities and should adapt to the available human team, the resources and the needs arising during healthcare. In the event of an emergency situation with a novice team, an autocratic position might be the most appropriate option. In contrast, in the event of a very complex scenario with a very experienced multidisciplinary team, the leader should be more open to listening to the comments and following the recommendations of the team.25–27
Management of stress and fatigueHumans are not machines, and our inherent nature implies that prolonged shifts and the lack of sleep expose healthcare professionals to tiredness, stress or distractions that favor the appearance of errors.
Tiredness and fatigue can affect analysis and decision-making, complex mental tasks and situational awareness.28,29 Sleep deprivation results in longer periods of ineffective, deficient and variable performance.30 As cognitive function decreases, we take longer to integrate information and there is a delay in executing a response. Likewise, fatigue secondary to long work shifts reduces alertness, slows the carrying out of tasks, and in sum hurts professional performance and patient safety.31
The scientific evidence points to a relationship between the level of stress and human performance.32,33 Although a degree of stress is necessary for healthcare professionals to stay alert and respond adequately in the face of an emergency, extreme stress levels hurt patient safety. On one hand, very low-stress levels lead to boredom and a lack of attention to tasks, while in contrast very high stress levels - often due to the work conditions and conflicts inherent to human interactions - lead to burnout syndrome, characterized by the following triad: emotional exhaustion, low professional performance, and depersonalization.32,33
Tools for training human skillsSince human error cannot be eliminated, effort must focus on identifying and minimizing error, making sure that people have adequate non-technical or human skills to deal with the risks and demands of their work.6
In recent decades, specific team training programs have been developed and implemented, seeking to optimize human skills (teamwork, communication, leadership, situation awareness, the assignment of roles and tasks, and decision-making) in order to secure a safe and efficient management of crisis situations.34
In the context of human skills, reference must be made to two of the methods most widely used and published in the literature35,36: Crisis Resource Management (CRM)37,38 and Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS®).39,40
Crisis Resource managementCrisis Resource Management (CRM) conceptualizes and contemplates the behavioral skills needed to optimize the performance of a clinical team to improve its precision, efficiency and adaptability, to guarantee patient safety.41,42
The main principles underlying CRM are closely related to those commented above in relation to non-technical skills.
CRM has been shown to have a significant influence in improving clinical team and patient communication, and in reducing the presence of adverse events. Nevertheless, the evidence of the impact of this methodology on patient evolution and mortality in the long term is not solid36,43.
TeamSTEPPSThis program was created in the United States in 2006 by the Agency for Healthcare Research and Quality (AHRQ) and the Department of Defense. It is under constant revision, and there is already a 3.0 version that can be consulted openly on the web.44
The main aim of the TeamSTEPPS is to integrate teamwork in clinical practice, being able to improve patient safety, promote a safety culture, and ensure quality and efficiency in patient care.45,46
The full program has three phases. The first phase evaluates the needs and identifies specific areas for improvement based on a standardized questionnaire developed by the AHRQ.47 The second phase involves TeamSTEPPS trainer education and posterior training of the participants from different Departments. Lastly, a third phase addresses maintenance and monitoring to integrate the methodology in clinical practice, and to diffuse the improvements in teamwork performance obtained by the TeamSTEPPS within the organization.48
Training is multimodal through scenarios, case studies, videos and clinical simulations. There are several course modalities in the second phase, involving a shorter course and another deeper and more extensive course.48
The main principles of the TeamSTEPPS are very similar to those of the CRM, including team structure (organization, definition of roles and responsibilities), leadership (coordination of the team, evaluation of its behavior, the assignment of tasks, team motivation), mutual support through adequate feedback, situational awareness (re-evaluation, anticipation) and communication.45
The main advantage of TeamSTEPPS is that the methodology used to implement the program is clear and homogeneous. It offers standardized checklists for assessing performance,49 along with concise work tools and clear cognitive aids for each of the aforementioned work areas.44
The TeamSTEPPS method is widely implemented at the international level. However, in Spain, and in contrast to the CRM, it has not been developed to the same extent, and few publications on this regard are available.45
With regard to the evidence of its benefits, several studies have shown that the TeamSTEPPS reduces the number of errors in the healthcare setting, with an increase in patient satisfaction.40,45
Behavior observation scalesIn addition to these human skill training programs, behavior observation scales have been introduced50–62 that can be used by qualified evaluators to objectively score the human skills of a group of healthcare professionals in a real or simulated scenario. Such behavior scales afford a common language to structure teaching, and serve as a basis for posterior debriefing. Most of these evaluation tools are designed to be used with multidisciplinary teams in real-life or simulated settings (Table 3. Behavior observation scales). Such instruments focus on two or more of the 5 most common human skill categories, i.e., communication, leadership and/or teamwork, situation awareness, decision making and task management. In choosing the most appropriate tool for the training of these skills in the management of critically ill patients, the teachers must select those that adapt best to the clinical setting in which the trainees are to be formed and also select those tools that have been previously validated.
Behavior observation scales.
| Scale name | Environment | Setting | Target subjects | References |
|---|---|---|---|---|
| Anaesthetists’ Non-Technical Skills (ANTS) | Operating room | Simulation and reality | Anesthetists | Fletcher et al. 200351Flin et al. 201052; 201153 |
| Oxford NOnTECHnical Skills (Oxford NOTECHS) | Operating room | Simulation and reality | Multidisciplinary (Operating room) | Mishra et al. 200954 |
| Non-Technical Skills for Surgeons (NOTSS) (60) | Operating room | Simulation and reality | Surgeons | Yule et al. 200855 |
| Ottawa CRM Global Rating Scale (Ottawa GRS) | Adults ICU/Emergencies | Simulation | Physicians | Kim et al. 200656 |
| Team Emergency Assessment Measure (TEAM) | Adults ICU/Emergencies | Simulation and reality | MultidisciplinaryICU/ Emergencies | Cooper et al. 201057 |
| Observational Skill-based Clinical Assessment Tool for Resuscitation (OSCAR) | Adults ICU/Emergencies | Simulation and reality | MultidisciplinaryICU/Emergencies | Walker et al. 201158 |
| Trauma NOTECHS(T-NOTECHS) | Adults ICU/Emergencies | Simulation and reality | MultidisciplinaryTrauma team | Steinemann et al. 201259Repo et al. 201960 |
| University of Texas Behavioral Markers for Neonatal Resuscitation (UTBMNR) | Pediatric ICU/Emergencies | Simulation and reality | MultidisciplinaryNeonatal team | Thomas et al. 200461 |
| Assessment of Obstetrical Team Performance (AOTP) | Obstetrics | Simulation | MultidisciplinaryObstetrical team | Tregunno et al. 200962 |
| Global Assessment of Obstetrical Team Performance (GAOTP) | Obstetrics | Simulation | MultidisciplinaryObstetrical team | Tregunno et al. 200962 |
In this training process we need a key element to implement such training programs, a teaching methodology that will serve as the basis: clinical simulation. There is general agreement that training in human skills essentially requires a safe learning context in which error should be seen as an opportunity to allow the trainees to improve as professionals and as persons, without placing the patient’s life at risk.63,64
ConclusionsIn summary, the science of the Human Factor is a discipline that seeks to design systems that make work more effective and efficient while guaranteeing safety by minimizing errors and supporting resilience in responding to the latter and to the unexpected events that may arise. Correct implementation of the Human Factor principles favors “making it easy to do things well and hard to do things wrong”, and that when errors do occur, they prove less likely to cause harm to patients.
Within the Human Factor, we have human skills that properly refer to people individually. The following have been identified in the literature as being the most important: decision-making, communication, teamwork and leadership, situational awareness and the management of stress and fatigue. Adequate training in these skills by healthcare professionals plays a key role in the care of the critically ill patient by complementing theoretical knowledge and the mastering of technical skills.
Financial supportThis study and its publication have received no financial support.
Conflicts of interestThe authors declare that they have no conflicts of interest.

