


Recently, the World Health Organization declared the novel coronavirus (2019-nCov) a global health emergency due to its global implications for the health care system and its economic impact. Italy was one of the first European countries with registered clustered cases of acute pneumonia. On February 23, 2020, the Italian government declared the first set of quarantine measures to slow the spread of the virus.1 Estimations show that 2019-nCoV is a high-diffusion virus with a 2% fatality rate; approximately 20% all hospital admissions were directly to the ICU.2 National health care systems could collapse if this spread of pneumonia continues at the current rate. This study aims to analyze official Italian data to build a predictive model.3 From February 23, 2020 to March 15, 2020, daily data from the cumulative reports of the Protezione Civile Italiana (Italian Civil Protection) were collected, including the number of positive subjects, hospital admissions, ICU admissions, deaths, and full recovery. Statistical programs were used for the analysis. Different models were tested, and forecast values were calculated, and the best model, with a p-value <0.05, was considered to calculate the predicted values. The number of positive subjects (PS) follows a non-linear regression with p<0.001 for the number of PS and hospital admissions, PS and ICU admissions, PS and deaths, and PS and recovered subjects. Simultaneously, the number of people admitted to hospitals follows a non-linear regression with p<0.001 (Table 1). Among the 46.7% of PS admitted in hospitals, 10.0% were admitted to the ICU. The ratio of hospitalized patients to those admitted to the ICU is 22.3%, the death rate is 5%, and the recovery rate is 8%. The relationship between hospital admissions and ICU admissions follows a linear regression, with p<0.001. Recent data on 2019-n CoV present different non-linear growth patterns, besides the rapidly increasing number of PS, which are very susceptible to public health rules. It is fascinating to observe the constant ratio of hospitalized and ICU admissions. If, in the next few weeks, infections reach 1% of the Italian population, over 60.000 ICU beds will be required, which may be the breaking point for the system. These results could be confirmed and highlighted by the increasing trend of ICU admissions, and the relationship between hospitalized patients and ICU admitted subjects. The national health care system needs more time to adapt to and deal with this challenge. The 2019 n-CoV transmission probability presents the following relationship. y = ax3bx2+cx + d. Here, y indicates infected subjects, x is the intrinsic potential reproducing number, and the constants a,b,c and d are the intercepts. With environmental strategies and adequate medical treatments, infection and death rates reduced, while recovery rates increased (Fig. 1a and b). Observing Italy's data, this equation is applicable to hospital and ICU admission, and to the rate of death and recovery. As in China, quarantine and environmental strategies have a positive, but slow effect. They can reduce the rate of infection, admissions to ICU, and death, and can change the model.4 Furthermore, this is a preliminary interpretation, and not the end of this phenomenon. It will be possible to analyze, customize, and fit the best model.5 However, in this context, it is important not to forget the emergency; necessary medical and surgical procedures should be guaranteed. A possible solution is to try to re-organize the mission of the hospital as happened in different and less dramatic events.6 This model has the potential to predict the worst-case scenario. With this knowledge, we are ready to do the best to prevent the system from reaching the breaking point and to change the 2019 nCoV curve now!
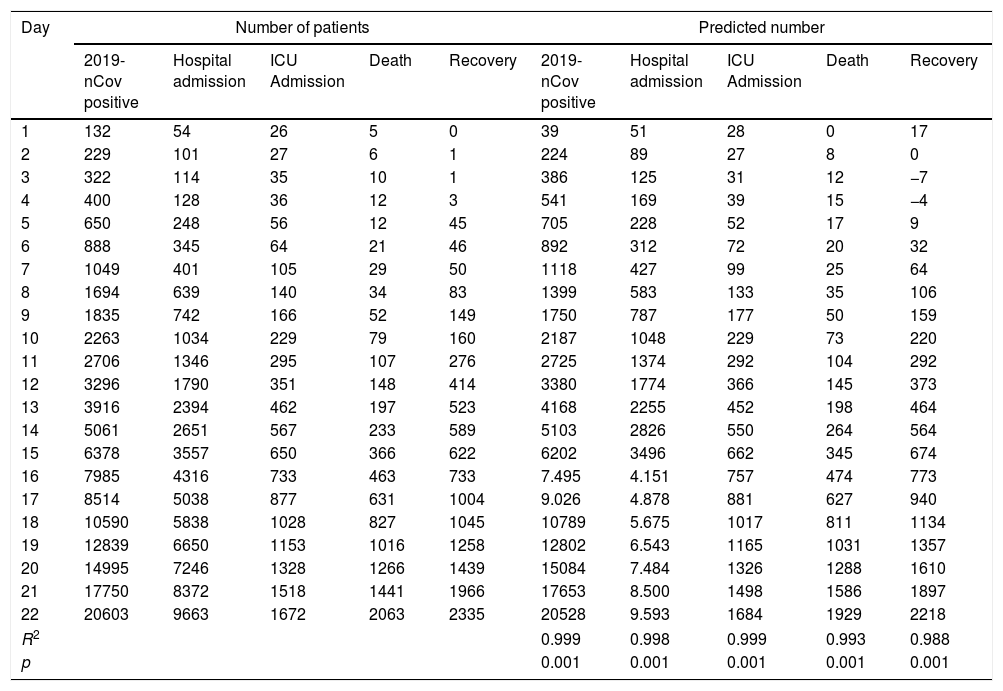
Data from February 23 until March 15, 2020. Left panel: number of 2019-nCov positive subjects, number of hospital admissions and ICU admissions, number of deaths, and recovery. Right panel: predicted mean value calculated using non- linear regression. R2 describes the goodness of fit, where 1 indicates a complete fit.
| Day | Number of patients | Predicted number | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2019-nCov positive | Hospital admission | ICU Admission | Death | Recovery | 2019-nCov positive | Hospital admission | ICU Admission | Death | Recovery | |
| 1 | 132 | 54 | 26 | 5 | 0 | 39 | 51 | 28 | 0 | 17 |
| 2 | 229 | 101 | 27 | 6 | 1 | 224 | 89 | 27 | 8 | 0 |
| 3 | 322 | 114 | 35 | 10 | 1 | 386 | 125 | 31 | 12 | −7 |
| 4 | 400 | 128 | 36 | 12 | 3 | 541 | 169 | 39 | 15 | −4 |
| 5 | 650 | 248 | 56 | 12 | 45 | 705 | 228 | 52 | 17 | 9 |
| 6 | 888 | 345 | 64 | 21 | 46 | 892 | 312 | 72 | 20 | 32 |
| 7 | 1049 | 401 | 105 | 29 | 50 | 1118 | 427 | 99 | 25 | 64 |
| 8 | 1694 | 639 | 140 | 34 | 83 | 1399 | 583 | 133 | 35 | 106 |
| 9 | 1835 | 742 | 166 | 52 | 149 | 1750 | 787 | 177 | 50 | 159 |
| 10 | 2263 | 1034 | 229 | 79 | 160 | 2187 | 1048 | 229 | 73 | 220 |
| 11 | 2706 | 1346 | 295 | 107 | 276 | 2725 | 1374 | 292 | 104 | 292 |
| 12 | 3296 | 1790 | 351 | 148 | 414 | 3380 | 1774 | 366 | 145 | 373 |
| 13 | 3916 | 2394 | 462 | 197 | 523 | 4168 | 2255 | 452 | 198 | 464 |
| 14 | 5061 | 2651 | 567 | 233 | 589 | 5103 | 2826 | 550 | 264 | 564 |
| 15 | 6378 | 3557 | 650 | 366 | 622 | 6202 | 3496 | 662 | 345 | 674 |
| 16 | 7985 | 4316 | 733 | 463 | 733 | 7.495 | 4.151 | 757 | 474 | 773 |
| 17 | 8514 | 5038 | 877 | 631 | 1004 | 9.026 | 4.878 | 881 | 627 | 940 |
| 18 | 10590 | 5838 | 1028 | 827 | 1045 | 10789 | 5.675 | 1017 | 811 | 1134 |
| 19 | 12839 | 6650 | 1153 | 1016 | 1258 | 12802 | 6.543 | 1165 | 1031 | 1357 |
| 20 | 14995 | 7246 | 1328 | 1266 | 1439 | 15084 | 7.484 | 1326 | 1288 | 1610 |
| 21 | 17750 | 8372 | 1518 | 1441 | 1966 | 17653 | 8.500 | 1498 | 1586 | 1897 |
| 22 | 20603 | 9663 | 1672 | 2063 | 2335 | 20528 | 9.593 | 1684 | 1929 | 2218 |
| R2 | 0.999 | 0.998 | 0.999 | 0.993 | 0.988 | |||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |||||
 Reports the model curve and its fitting curve of positive subjects of 2019-nCov, hospital and ICU admissions, death, and recovery. (b) Reports the ICU admission trend with a moving averages relation.")
None declared.
The Study follows Strobe Guidelines.
Database: data are available on http://www.protezionecivile.gov.it/attivita-rischi/rischio-sanitario/emergenze/coronavirus.
Statistic calculate were performed using Microsoft Excel® and STATA 16® program (STATA Corp LP 4905 Lakeway Drive TX 77845 USA by a physician (with statistic competence) and by an engineer: all calculate were attached as supplementary file.
Author contributionsMelegari G and Barbieri A: concept design of the study, statistic calculate, Maini G: statistic calculate and control, Giuliani E: writing of the paper, Barbieri L: graphical aspects, Baffoni P and Bertellini E: manuscript revision and final approval.
KeypointsThe study analyzes the Italian Novel Coronavirus (2019-nCov) outbreaks, searching possible predicting model, underlining the risk of the trend of phenomena.
Conflict of interestNone.
Special thanks to Dr. Giuliano Carrozzi, Epidemiology Azienda AUSL Modena, Italy.
The following are the supplementary data to this article:


