





A 53-year-old-caucasian man, ex-smoker, with past medical history of dyslipidaemia had an out-of-hospital successful cardiopulmonary resuscitation after cardiac arrest in ventricular fibrillation (VF) due to an anterior ST-elevation myocardial infarction (STEMI). A primary percutaneous coronary intervention (PCI) was performed with revascularization of the left anterior descending artery (LAD) using a drug eluting stent. The pre-discharge echocardiogram showed a left ventricular ejection fraction (LEVF) of 40%. The patient was discharged at 6th day.
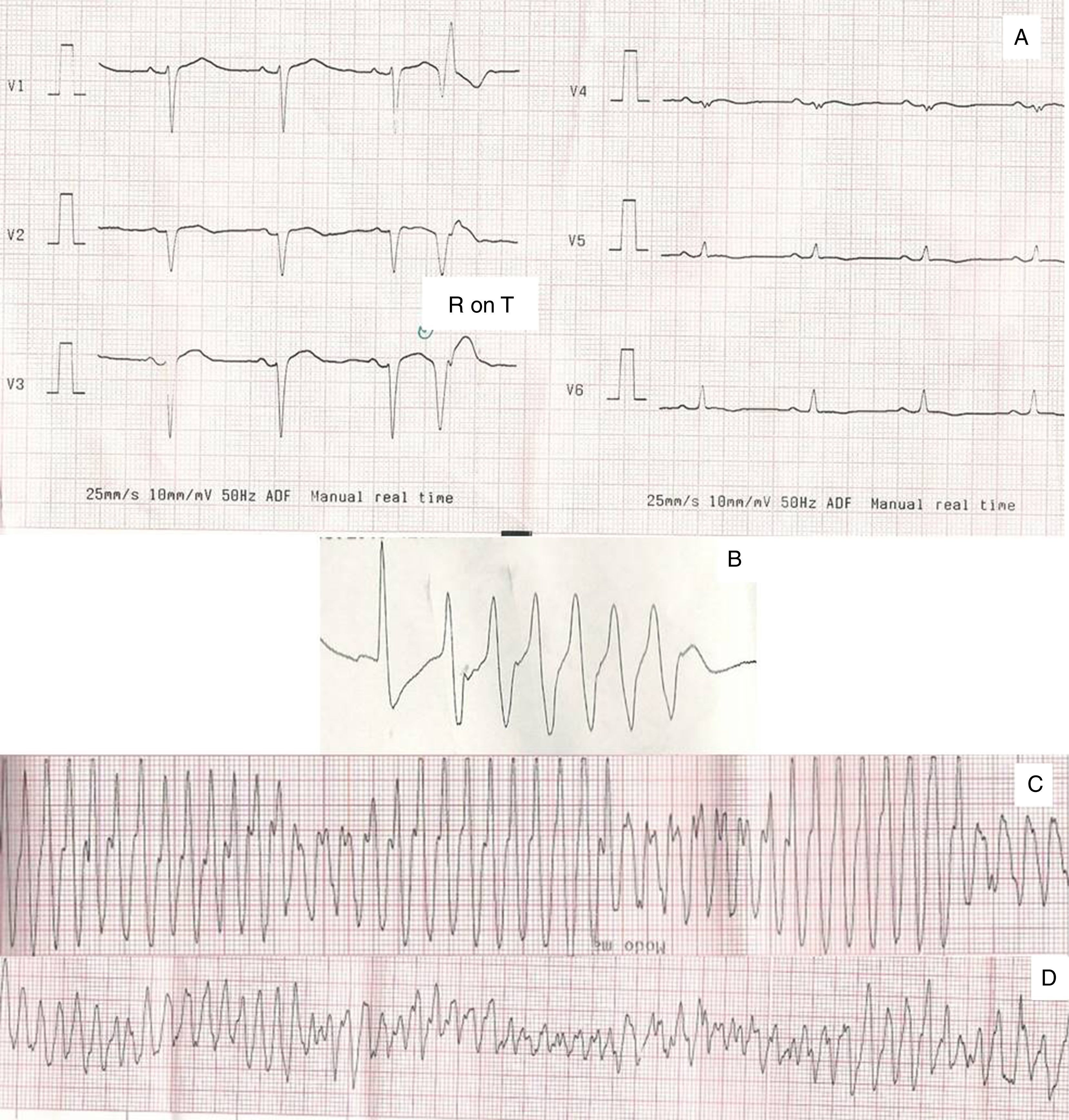
Five days later the patient was resuscitated after another cardiac arrest with documented VF. A repeated coronary angiography revealed acute LAD stent thrombosis. A “stent in stent” PCI of LAD was successfully performed. In the following hours the patient evolved into cardiogenic shock with a LVEF of 20%. Aminergic and inotropic support was started with norepinephrine, dopamine and dobutamine, as well as intra-aortic balloon pump and invasive mechanical ventilation. On the second day of hospitalization the patient presented several episodes of polymorphic ventricular tachycardia (VT), triggered by premature ventricular complexes (VPC), that rapidly degenerated into VF (Fig. 1). PR, QRS and QT intervals were normal. Intravenous amiodarone, esmolol, lidocaine, magnesium and midazolam were administered. Despite maintaining of combined antiarrhythmic drugs (AAD) ventricular tachyarrythmias persisted, exhibiting the same pattern for VT/VF initiation.
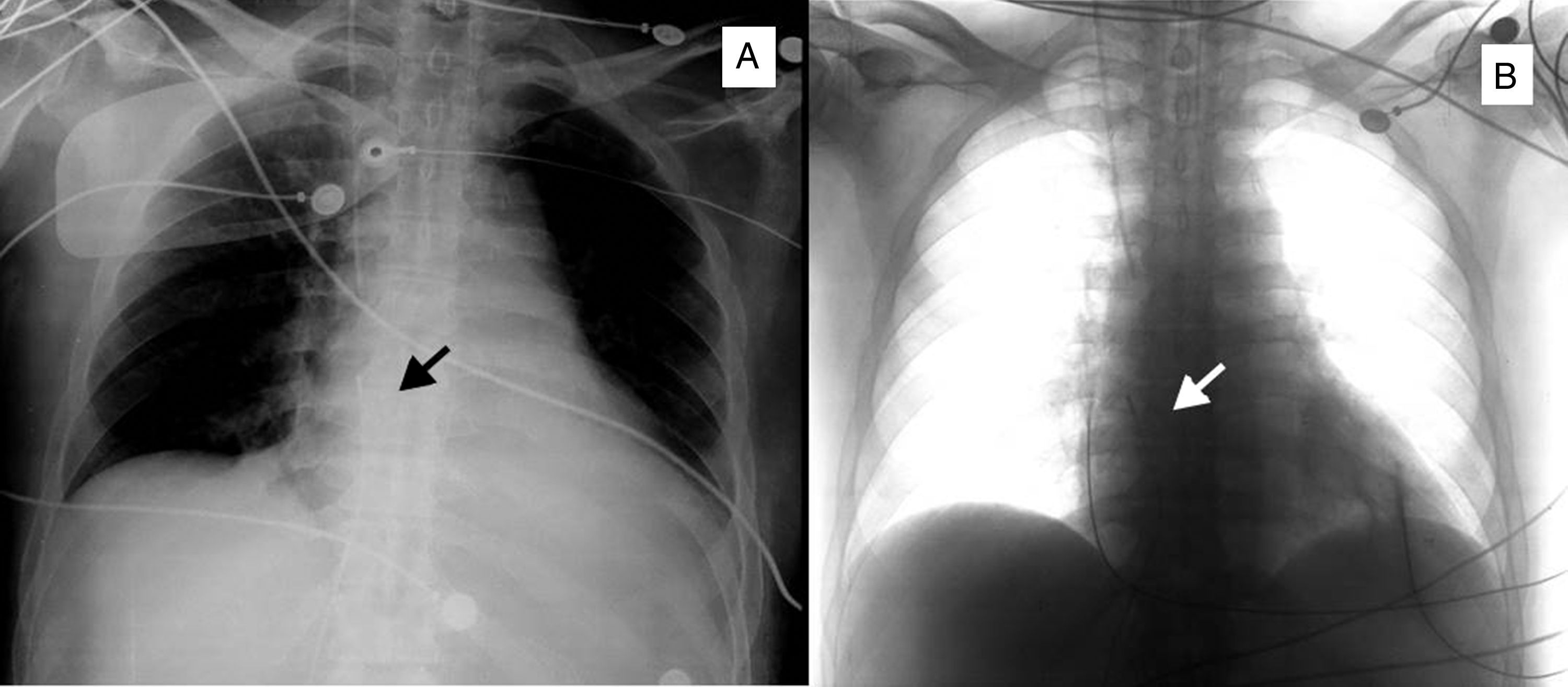
In order to suppress premature ectopic beats, it was decided to perform atrial overdrive pacing. This was accomplished by using a temporary pacemaker, programmed at 85bpm (heart rate before pacing was 60 beats per minute), with an active fixation catheter (Biotronik TC-116-Screw) placed in the right atrial appendage, by femoral approach (Fig. 2).
After starting atrial pacing there was a complete suppression of VPC and no more VT episodes were observed. AAD were progressively weaned off while maintaining atrial pacing at the same rate and, although lidocaine was discontinued and amiodarone switched to an oral regimen, neither VPC nor VT/VF recurred. The electrocatheter was removed on the 8th day after implantation (four days after suspension of lidocaine and switching of amiodarone to oral regimen). Before discharge, the patient underwent a dual-chamber ICD implantation with the pacing rate programmed at 80bpm, and two zones of tachycardia detection and corresponding therapies (VT zone: at 170bpm; VF zone: at 210bpm).
DiscussionThe incidence of sustained ventricular arrhythmias (VA) in acute coronary syndromes (ACS) is 5–10%.1 In the context of ischaemia, VPC, VT and VF can be secondary to an automatic or reentrant mechanism.1,2 Myocardial ischaemia leads to changes in the ionic imbalance of cardiomyocytes, resulting in shorter duration of the action potential and less negative resting membrane potential.1 In this condition early and delayed triggers after depolarization may occur, inducing VPC and arrhythmogenic currents, especially from the ischaemic/reperfused to the non-ischaemic areas.1,2
In our patient the VPC provoked “R-on-T” phenomenon, resulting in recurrent episodes of VT and VF (Fig. 1).
Amiodarone blocks the depolarizing sodium currents and potassium channels responsible for conduction of repolarizing currents inhibiting ventricular arrhythmias (VA) by influencing automaticity and re-entry,3,4 and esmolol blocks sympathetic mediated triggering mechanisms underlying VA.2,5 Despite the combined AAD therapy, the patient maintained recurrent episodes of VT/VF and perfusion of lidocaine was started without obtaining electrical stability.2,3,6
Temporary overdrive pacing has been pointed as an option for drug resistant ventricular arrythmias.7,8 In recent European Society of Cardiology's Guidelines for the management of ventricular arrhythmias, transvenous catheter overdrive stimulation received a class IIa of recommendations, level of evidence C, in cases of recurrent VA despite the use of anti-arrhythmic drugs.3
Lower heart rate results in increased ventricular repolarization heterogeneity and increases the possibility of an ectopic ventricular complex reaching reentrant tissue after refractory period. The heart rate increases with temporary pacing, shortens the interval between beats and decreases the likelihood of appearance of premature ventricular complexes and increases the likelihood of these reaching pro-arrhythmic tissue in refractory period.
As right ventricular pacing can be deleterious for ventricular systolic function, and this patient presented a severe impairment in LVEF without evidence of atrio-ventricular conduction disturbances, electrical stimulation was performed in an uncommon way, using an active fixation temporary pacing catheter placed in the right atrium. The aim was to obtain intrinsic atrioventricular conduction with a narrow QRS and avoid the deleterious effect of ventricular pacing in a patient with cardiogenic shock.
Temporary pacing with an active fixation catheter is designed to allow ventricular septal pacing, but alternative pacing points can also be obtained with this type of catheter. Attention should be given while placing this lead in locations other than ventricular septum. Positioning in the atrial septum could be safer and avoid potential complications in patients where any perforation can be a severe complication. The femoral approach may facilitate positioning of the lead in an atrial positioning but, due to longer intravenous trajectory and the exposed fixation helix, the right jugular approach may be preferred.
The use of non-active fixation temporary pacing leads for atrial pacing might be also considered but the risk of dislodgement is high.
In conclusion, temporary atrial overdrive pacing is an effective and safe treatment for resistant electrical storm in patients with severe impairment of left ventricular systolic function.
Conflict of interestThe authors have no disclosures.

