





To assess the predictive capacity of the Rapid Shallow Breathing Index (RSBI) for success in spontaneous breathing trials (SBT) and extubation in critically ill patients. We evaluated the association between RSBI, duration of mechanical ventilation, and ventilator-free time at 28 days.
DesignProspective multicenter observational study. Secondary analysis of the COBRE-US study.
SettingIntensive care unit (ICU).
Patients or participants367 patients in the ICU receiving invasive mechanical ventilation.
InterventionsAssessment of RSBI at the end of SBT.
Main variables of interestRSBI, SBT, duration of mechanical ventilation, and ventilator-free time at 28 days were evaluated.
Results367 patients in the ICU under invasive mechanical ventilation were evaluated, of whom 59.7% were male with a median age of 61 years (IQR: 49–72). A total of 456 SBT were conducted with a success rate of 76.5%. RSBI had a ROC-curve of 0.53 for SBT success and a ROC-curve of 0.48 for extubation. The Spearman correlation coefficient between RSBI and duration of ventilation was 0.117 (p = 0.026), while for ventilator-free time at 28 days, it was −0.116 (p = 0.028).
ConclusionsRSBI was not associated with success in SBT or extubation, regardless of the cutoff point used. Correlation analyses showed weak associations between RSBI and both the duration of ventilation and ventilator-free time at 28 days.
Evaluar la capacidad predictiva del Índice de Respiración Superficial Rápida (IRSR) para el éxito en la prueba de respiración espontánea (PRE) y extubación en pacientes críticamente enfermos. Se evaluó la asociación entre IRSR, la duración de la ventilación mecánica y el tiempo libre de ventilador a los 28 días.
DiseñoEstudio observacional prospectivo multicéntrico. Análisis secundario del estudio COBRE-US.
ÁmbitoUnidad de cuidados intensivo (UCI).
Pacientes o participantesPacientes en la UCI recibiendo ventilación mecánica invasiva.
IntervencionesEvaluación del IRSR al finalizar la PRE.
Variables de interés principalesSe evaluaron IRSR, PRE, duración de la ventilación mecánica y tiempo libre de ventilador a los 28 días.
ResultadosSe evaluaron 367 pacientes en la UCI bajo ventilación mecánica invasiva, de estos el 59.7% eran de sexo masculino con una mediana de edad de 61 años (RIC: 49–72). Se realizaron 456 PRE con tasa de éxito del 76.5%. El IRSR presenta una curva ROC de 0,53 para éxito del PRE y una curva ROC de 0.48 para extubación. El coeficiente de correlación de Spearman entre la IRSR y la duración de la ventilación fue de 0.117 (p = 0,026), mientras que para el tiempo libre de ventilación a los 28 días fue de −0.116 (p = 0.028).
ConclusionesEl IRSR no se asoció con la PRE ni en la extubación, independiente del punto de corte utilizado. Los análisis de correlación mostraron asociaciones débiles entre IRSR y tanto la duración de la ventilación como el tiempo libre de ventilador a los 28 días.
Invasive mechanical ventilation (IMV) is employed as a therapy for various diseases compromising alveolar oxygen diffusion capacity.1 Its primary objective is to facilitate the mechanical ventilation process, partially or completely alleviating physical effort and improving gas exchange in critically ill patients in intensive care unit (ICU).1–5 Predicting success in the weaning process from IMV is crucial for clinical decision-making in ICU. Success is defined as transitioning to spontaneous ventilation without the need for reintubation for at least 48 h after extubation.2 However, failures in this procedure are common and can significantly increase complication rates, mortality, and healthcare costs. Therefore, it is essential to employ clinical tests to estimate the probability of failure or success in this process.1,4,5 Among these tests are the rapid shallow breathing index (RSBI), leak test, diaphragmatic ultrasound measurements, and objective cough measurements, which allow prediction of success in spontaneous breathing trials (SBT) or extubation.6–8
The RSBI, as first outlined by Yang and Tobin in 1991, underwent assessment in a cohort of 100 ICU patients who were hemodynamically stable.9 Their analysis revealed that an RSBI below 105 breaths per minute per liter (breaths/min/L) was indicative of successful extubation, demonstrating a sensitivity of 97% and specificity of 64%.9 Jacob et al. assessed the relationship between respiratory rate and tidal volume and found that its measurement at baseline and after 30 min of weaning is more predictive of weaning outcome than negative inspiratory force and minute volume.10 A meta-analysis conducted by Jia et al., with a sample of 13170 patients, found that the RSBI has a sensitivity of 60%, a specificity of 68%, and an area under the receiver operating characteristic curve (ROC curve) of 0.814 to predict extubation success.11 The authors concluded that the included studies could neither confirm nor discard the use of RSBI as a single parameter for predicting successful extubation.11
Despite significant advancements in clinical research on the weaning time of IMV and the use of bedside clinical tests, certain limitations persist, hindering the improvement of success rates in weaning and extubation.6,9,12 Although the RSBI is widely utilized in the ICU, there is a scarcity of medical evidence describing its predictive capacity when employing different cutoff points in a heterogeneous population.9–13 Therefore, our aim is to describe the predictive capacity of RSBI, employing different cutoff points, regarding success in SBT and extubation in critically ill patients. Additionally, we will assess its association with variables such as duration of mechanical ventilation. This secondary analysis is part of the COBRE-US study.13
Patients and methodsProspective multicenter observational study. Secondary analysis of the COBRE-US study.
PopulationThe study included adult patients undergoing weaning process, admitted to four ICU located at Fundación Cardioinfantil-Instituto de Cardiología, Fundación Neumológica Colombiana, and Fundación Clínica Shaio in Bogotá, Colombia. Data collection was conducted from February 2019 to November 2021.
Participants selected for the study were adults requiring IMV for more than 48 h and meeting criteria to initiate the weaning process. These criteria included robust cough, absence of respiratory secretions, resolution of the acute phase of the disease leading to endotracheal intubation, stable cardiovascular condition (heart rate <140/min, systolic blood pressure 90−160 mmHg), none or low-dose vasopressor support (norepinephrine ≤0.1 mcg/kg/min or dobutamine ≤5 mcg/kg/min), adequate metabolic status (pH > 7.35 and ≤7.48 in acid-base balance, electrolytes within normal ranges such as phosphorus, sodium, and potassium), temperature ≤38 °C, hemoglobin >7 g/dl (>10 g/dl in patients with coronary disease), a Glasgow Coma Scale score >12, and absence of delirium according to the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Additionally, adequate oxygenation was required, with oxygen saturation (SaO2) above 90% with an inspired oxygen fraction (FiO2) ≤0.4, a ratio of arterial oxygen partial pressure to inspired oxygen fraction (PaO2/FiO2) greater than 150 mmHg, and positive end-expiratory pressure (PEEP) ≤8 cm H2O. Pregnant patients, those with neuropsychiatric diseases, or diaphragmatic paralysis were excluded from the study.
MeasurementsSBT: The patient underwent a 30-minute SBT using a T-piece or pressure support ventilation (PSV). The trial could be stopped in case of intolerance. Failure was defined as the presence of at least one of the following criteria: PaO2 ≤ 60 mmHg or SpO2 ≤ 90% with FiO2 ≥ 0.50, PaCO2 > 50 mmHg or increase of >8 mmHg from baseline, pH < 7.32 or decrease of > 0.7 units, respiratory rate ≥ 35/min or increase ≥50% from baseline, heart rate ≥140 bpm or increase ≥20% from baseline, systolic blood pressure >180 or increase ≥20% or systolic blood pressure <90 mmHg. Additional criteria included the development of de novo cardiac arrhythmias, abrupt change in mental status; onset of tachycardia HR > 140 per min or bradycardia HR < 60 per min; or presence of two or more signs of respiratory distress such as increased respiratory effort, use of accessory muscles, paradoxical abdominal movement, facial signs of distress, diaphoresis, cyanosis, and marked dyspnea.5,7,13
The RSBI, calculated as respiratory rate (number of breaths per minute) divided by Tidal Volume in liters (f/VT), was evaluated immediately after cuff leak test during transition to spontaneous mode. A value less than 105 breaths/min/L was considered a favorable test.8
In addition to test results, we collected information on other variables, including age, sex, admission diagnosis, etiology of respiratory failure, arterial blood gases before extubation (including pH, PCO2, HCO3, PO2, FiO2), ventilatory mode during weaning process, ventilatory mode used during weaning (pressure support or T-Piece), duration of mechanical ventilation, ventilator-free days at 28 days, duration of weaning process (time from initiation of weaning process or mode change until final extubation), days from ICU admission to initiation of weaning process, and total days of ICU stay.
OutcomesThe primary objective of our research was to evaluate the predictive capacity of RSBI to determine success or failure of SBT and extubation. Failure in SBT was characterized by clinical variables, while in the case of extubation, it was defined as the need for reintubation within 48 h following extubation. Absence of reintubation was considered indicative of successful weaning process. We evaluated the association between RSBI, duration of mechanical ventilation, and ventilator-free time at 28 days.
Ethical considerationsThe studies involving human participants were reviewed and approved by the Ethics Committee of Fundación Neumológica Colombiana (approval number 201806-23607). Prior to participating in the study, all participants provided written informed consent, and the confidentiality of their data was strictly maintained throughout the study.
Statistical analysisData were transcribed into Research Electronic Data Capture (REDCap) software14 and analyzed in Stata version 16 (StataCorp LLC, College Station, USA). Continuous variables were presented as mean (standard deviation) or median (interquartile range) depending on their distribution, while categorical variables were presented as absolute and relative frequencies. Distribution of continuous variables was assessed, and t-test or Mann–Whitney U test were applied for normally distributed and non-normally distributed variables, respectively. Categorical variables were compared using Chi2 test or Fisher's exact test, as appropriate, based on frequencies in the contingency table.
A ROC-curve was constructed to evaluate the predictive capacity of RSBI in predicting success in SBT and extubation. Additionally, it was stratified by RSBI cutoff points, with values below 80, between 80 and 105, and above 105 breaths/min/L. We calculated the association between RSBI, duration of mechanical ventilation, and ventilator-free time at 28 days using Spearman correlation coefficient. We based our sample size calculations on the methodology employed in the COBRE-US trial conducted by Varón-Vega et al.13 A p-value less than 0.05 was considered statistically significant. All analyses were performed using Stata version 17 (StataCorp LLC, College Station, USA).
ResultsA total of 367 patients in the ICU receiving invasive mechanical ventilation were included. Among these, 59.7% were males, with a median age of 61 years (IQR 49–72). The most common reasons for ICU admission were ventilatory failure due to hypoxemia, followed by shock and hypercapnia, present in 75%, 14.9%, and 6.6% of cases, respectively (Table 1).
Characteristics of the patients.
| Number of patients n(%) | 367 (100) |
|---|---|
| Male, n (%) | 219 (59.7) |
| Age in years, median (IQR) | 61 (49–72) |
| Weight Kg, median (IQR) | 70 (60–80) |
| Height cm, mean (SD) | 163.6 (10) |
| Body mass index kg/m2, Median (IQR) | 25.3 (21.7–29.1) |
| Active Smoking, n (%) | 33 (9) |
| Active alcoholism, n (%) | 22 (6) |
| Reason for ICU admission, n (%) | |
| Medical | 345 (94) |
| Surgical (only postsurgical) | 22 (6) |
| Duration of ventilation in days, median (IQR) | 10.7 (9.3−12.2) |
| Type of ventilatory failure, n (%) | |
| Shock | 52 (14.9) |
| Hypercapnia (pH < 7.25, high CO2) | 23 (6.6) |
| Hypoxemia (PaO2 < 60, usual FiO2) | 261 (75) |
| Neuromuscular | 2 (0.6) |
| Perioperative | 10 (2.9) |
| Comorbidities, n (%) | |
| Diabetes Mellitus | 113 (30.8) |
| Hypertension | 173 (47.1) |
| Asthma | 8 (2.2) |
| Pulmonary fibrosis | 6 (1.6) |
| Chronic kidney disease | 69 (18.8) |
| Chronic liver disease | 17 (4.6) |
Notes: IQR: interquartile range, SD: standard deviation, Kg: kilograms, cm: centimeters, ICU: intensive care unit. CNS: central nervous system.
The main comorbidities observed were systemic arterial hypertension, diabetes mellitus, and chronic kidney disease, found in 47.1%, 30.8%, and 18.8% of patients, respectively. During this period, 456 SBTs were conducted, with a success rate of 76.5%. RSBI had a median of 56 breaths/min/L (IQR 43–75) (Table 2).
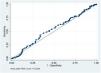
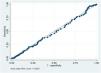
RSBI showed a ROC curve of 0.53 (95% CI: 0.50−0.55; p = 0.161) for predicting SBT success and 0.48 (95% CI: 0.46−0.50; p = 0.317) for predicting extubation success (Figs. 1 and 2). The Spearman correlation coefficient between RSBI and duration of ventilation was 0.117 (p = 0.026), while for ventilator-free time at 28 days, it was −0.116 (p = 0.028) (Supplementary Figures).


In a bivariate model exploring test thresholds, RSBI for extubation success probability showed ROC curves of 0.47, 0.41, and 0.38 for scores below 80, between 80 and 105, and above 105, respectively (Supplementary Figures). Additionally, when evaluating SBT success possibility with RSBI according to scores below 80, between 80 and 105, and above 105, ROC curves of 0.45, 0.45, and 0.36 were observed, respectively (Supplementary Figures).
DiscussionIn this secondary analysis of the COBRE-US trial, we extend existing medical evidence regarding the predictive capacity of RSBI in critically ill patients under mechanical ventilation, highlighting limited predictive ability for SBT and extubation success. Correlation analyses reveal statistically significant but weak associations between RSBI and both ventilation duration and ventilator-free time at 28 days.
Yang et al.9 demonstrated high predictive capacity in the weaning process using the f/VT ratio, with an ROC curve of 0.89. Furthermore, they noted that this measure is easy to calculate, independent of patient effort and cooperation, has significant predictive power, and has a threshold value of 105, easy to remember. In addition, subsequent studies have revealed poor predictive capacity when using values of 100 or close to predict extubation success.15 Karthika et al. showed that the rate of change in RSBI between the start and end of a 120-minute SBT could be a better predictor of extubation outcome than a single RSBI measured at the end of the SBT in mechanically ventilated patients, achieving an ROC curve of 0.933, sensitivity of 91%, and specificity of 86%.16 Our results differ from those described previously, which could be attributed to factors associated with diverse ICU populations, prolonged mechanical ventilation, elderly patients, and different RSBI cutoff points evaluated.9,17–21
Currently, there is a discussion about what the optimal cutoff point for RSBI is with the highest predictive capacity for extubation success.9,19,22–24 Goncalves et al.22 have reported that a cutoff point ≤78 breaths/min/L showed good capacity to differentiate patients undergoing more than 72 h of mechanical ventilation who could be successfully extubated, with an area under the ROC curve of 0.74. In our study, patients had an average duration of ventilation of 10.7 days, with a median RSBI of 56 breaths/min/L. However, none of the RSBI cutoff points used proved to be useful in predicting failed extubation.
A meta-analysis conducted by Trivedi et al.21 examined 48 studies involving RSBI measurements in 10,946 patients. The results indicated that an RSBI value <105 had a sensitivity of 83% (95% CI: 0.78−0.87) for predicting extubation success, with a specificity of 58% (95% CI: 0.49−0.66) and a diagnostic odds ratio of 5.91 (95% CI: 4.09–8.52). In the range of 80–105, the sensitivity was 83% (95% CI: 0.77−0.88), specificity was 54% (95% CI: 0.42−0.67), and the diagnostic odds ratio was 5.30 (95% CI: 3.15–8.92). For RSBI < 80, the sensitivity was 84% (95% CI: 0.75−0.90), specificity was 62% (95% CI: 0.53−0.70), and the diagnostic odds ratio was 7.43 (95% CI: 4.17–13.21). These findings remained consistent across multiple subgroup analyses reflecting different patient characteristics and operational variations in RSBI measurement. According to our findings, regardless of the cutoff point used, the index results were poor, suggesting the need to combine RSBI with other bedside tests.11,21
In our study, we have found a weak positive correlation between the RSBI index and the duration of ventilation. This finding suggests that patients undergoing prolonged mechanical ventilation may face challenges in the weaning process, which is reflected in higher RSBI values.20,25 This result is supported by a weak negative correlation between the RSBI index and ventilator-free time at 28 days in our data.
LimitationsThe strengths of this study lie in its prospective, multicenter design, investigating the predictive capacity of RSBI in critically ill patients before extubation. Although based on observational methodology and data collection from clinical records, our research team has extensive experience in the interpretation, extraction, and appropriate synthesis of this type of data, allowing us to address methodological challenges with solidity and rigor.
The ICU therapist assessed RSBI immediately after cuff leak test during transition to spontaneous mode. These therapists received standardized training to perform this measurement and were not informed about the successful or unsuccessful outcome of SBT. The patient cohort included a heterogeneous variety of medical and surgical diseases, without subcategorization, influencing underlying respiratory mechanics and the outcome of RSBI predictive capacity. Further studies are needed to complement the evaluation of RSBI with other clinically validated tests, different cutoff points, and patients with various diseases to enhance its diagnostic accuracy and reliability.
In conclusion, RSBI was not associated with success in SBT or extubation, regardless of the cutoff point used. Correlation analyses show weak associations between RSBI and ventilation duration, as well as ventilator-free time at 28 days. It is suggested that RSBI not be used as the sole criterion for determining extubation, but rather as a complement to other validated tests performed at the patient's bedside in the ICU.
Author contributionsFabio Varón-Vega, Eduardo Tuta-Quintero, Henry Robayo-Amortegui, Adriana Rincón, Luis F. Giraldo-Cadavid, and Pablo Monedero: study design and structure.
Jonathan Palacios, Stephanie Crevoisier, Diana C. Duarte, Marcela Poveda, and Laura Cucunubo: data collection.
Fabio Varón-Vega, Eduardo Tuta-Quintero, Henry Robayo-Amortegui, Adriana Rincón, and Luis F. Giraldo-Cadavid: data analysis and manuscript writing.
Competing interestsThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
FundingThis work was supported by Ministerio de Ciencia Tecnología e Innovación (Grant: 335980763260) and Universidad de La Sabana (Grant: MED-253-2019).
The authors are most thankful for the Universidad de La Sabana, Fundación Cardioinfantil-Instituto de Cardiología, Fundación Neumológica Colombiana, Fundación Clínica Shaio y Universidad de Navarra.
The following is Supplementary data to this article:


