

The first COVID-19 wave caused by SARS-CoV-2 helped us to understand the course of this previously unknown disease, with its particular characteristics – including very severe acute respiratory distress syndrome (ARDS), a need for deep sedation and neuromuscular block, maneuvering in prone decubitus, an increased risk of thrombotic events, and prolonged mechanical ventilation.1 The data obtained from different studies made during that period led to subsequent changes in the management strategy applied to critical patients with COVID-19. In this regard, the inefficacy of antivirals such as lopinavir and ritonavir, as well as of hydroxychloroquine, appears to have been confirmed.2,3 On the other hand, remdesivir could offer some benefit in shortening the duration of symptoms in patients with more milder forms of the disease, but does not seem to significantly modify the course of severe COVID-19 or reduce the mortality rate.4 More controversial data have been obtained in relation to tocilizumab in terms of the lowering of mortality or reduction of the severity of COVID-19.5 On the other hand, with regard to the potential impact of corticosteroid use upon the course of patients infected with SARS-CoV-2, the RECOVERY6 trial is one of the most consistent studies available to date.
It therefore seems reasonable to assume that the experience gained in the course of the first wave, and the availability of data on the different treatments used on an experimental basis during that period, may have contributed to a different management approach to critical COVID-19 patients admitted during the second wave of the pandemic, with modification of the clinical outcomes.
We retrospectively analyzed the characteristics of all the patients admitted with SARS-CoV-2 infection to the Intensive Care Unit (ICU) of a third-level university hospital in Spain in the period between 15 March and 5 December 2020. All patients admitted up until 7 June were regarded as corresponding to the first wave of the pandemic, while all those admitted from 21 July onwards were taken to correspond to the second wave. We evaluated patient age and gender, comorbidities, laboratory test data, the need for ventilatory support, the medication prescribed (corticosteroid use was recorded on a dichotomic basis as either No or Yes, if the patient received at least 40 mg of methylprednisolone or its equivalent, during a period of at least 5 days to treat the inflammation associated to viral pneumonia), the duration of stay, and the mortality rate at 28 days.
The data were obtained through the COVID-19 patients registry of the Department of Intensive Care Medicine, following approval by the local Research Ethics Committee and the obtainment of written and/or telephone consent from the patients or their representatives.
A descriptive analysis was made of the study sample, reporting categorical variables as percentages, and continuous quantitative variables as the mean and standard deviation (SD). Comparisons between groups were made using the Pearson chi-squared test or the Fisher exact test for the comparison of proportions, while the Student t-test for independent samples with or without Welch correction was used for the comparison of means.
A total of 254 patients were admitted during the study period. We excluded 28 patients in which SARS-CoV-2 infection was not confirmed. A total of 228 patients were analyzed, of which 68 corresponded to the first wave of the pandemic and 160 to the second wave.
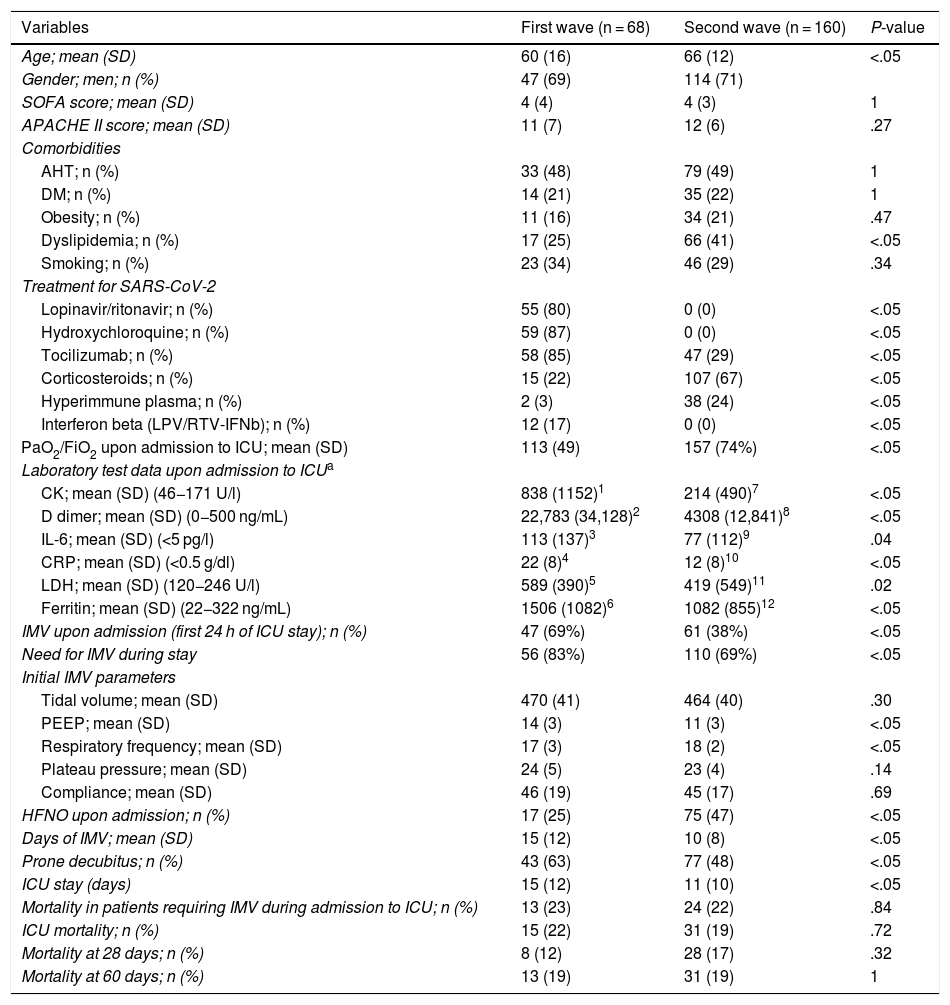
The patients of the first wave were significantly younger than those of the second wave (mean difference = 6 years (95%CI: 2.20–9.80); P < .05). Significant differences were also observed in the specific anti-COVID-19 medication prescribed, with an increased use of corticosteroids (22% versus 67%; P < .05) and hyperimmune plasma (3% versus 24%; P < .05) in the second wave (Table 1).
Comparison of the patients admitted to the ICU during the two waves of the pandemic due to confirmed disease secondary to SARS-CoV-2 infection.
| Variables | First wave (n = 68) | Second wave (n = 160) | P-value |
|---|---|---|---|
| Age; mean (SD) | 60 (16) | 66 (12) | <.05 |
| Gender; men; n (%) | 47 (69) | 114 (71) | |
| SOFA score; mean (SD) | 4 (4) | 4 (3) | 1 |
| APACHE II score; mean (SD) | 11 (7) | 12 (6) | .27 |
| Comorbidities | |||
| AHT; n (%) | 33 (48) | 79 (49) | 1 |
| DM; n (%) | 14 (21) | 35 (22) | 1 |
| Obesity; n (%) | 11 (16) | 34 (21) | .47 |
| Dyslipidemia; n (%) | 17 (25) | 66 (41) | <.05 |
| Smoking; n (%) | 23 (34) | 46 (29) | .34 |
| Treatment for SARS-CoV-2 | |||
| Lopinavir/ritonavir; n (%) | 55 (80) | 0 (0) | <.05 |
| Hydroxychloroquine; n (%) | 59 (87) | 0 (0) | <.05 |
| Tocilizumab; n (%) | 58 (85) | 47 (29) | <.05 |
| Corticosteroids; n (%) | 15 (22) | 107 (67) | <.05 |
| Hyperimmune plasma; n (%) | 2 (3) | 38 (24) | <.05 |
| Interferon beta (LPV/RTV-IFNb); n (%) | 12 (17) | 0 (0) | <.05 |
| PaO2/FiO2 upon admission to ICU; mean (SD) | 113 (49) | 157 (74%) | <.05 |
| Laboratory test data upon admission to ICUa | |||
| CK; mean (SD) (46−171 U/l) | 838 (1152)1 | 214 (490)7 | <.05 |
| D dimer; mean (SD) (0−500 ng/mL) | 22,783 (34,128)2 | 4308 (12,841)8 | <.05 |
| IL-6; mean (SD) (<5 pg/l) | 113 (137)3 | 77 (112)9 | .04 |
| CRP; mean (SD) (<0.5 g/dl) | 22 (8)4 | 12 (8)10 | <.05 |
| LDH; mean (SD) (120−246 U/l) | 589 (390)5 | 419 (549)11 | .02 |
| Ferritin; mean (SD) (22−322 ng/mL) | 1506 (1082)6 | 1082 (855)12 | <.05 |
| IMV upon admission (first 24 h of ICU stay); n (%) | 47 (69%) | 61 (38%) | <.05 |
| Need for IMV during stay | 56 (83%) | 110 (69%) | <.05 |
| Initial IMV parameters | |||
| Tidal volume; mean (SD) | 470 (41) | 464 (40) | .30 |
| PEEP; mean (SD) | 14 (3) | 11 (3) | <.05 |
| Respiratory frequency; mean (SD) | 17 (3) | 18 (2) | <.05 |
| Plateau pressure; mean (SD) | 24 (5) | 23 (4) | .14 |
| Compliance; mean (SD) | 46 (19) | 45 (17) | .69 |
| HFNO upon admission; n (%) | 17 (25) | 75 (47) | <.05 |
| Days of IMV; mean (SD) | 15 (12) | 10 (8) | <.05 |
| Prone decubitus; n (%) | 43 (63) | 77 (48) | <.05 |
| ICU stay (days) | 15 (12) | 11 (10) | <.05 |
| Mortality in patients requiring IMV during admission to ICU; n (%) | 13 (23) | 24 (22) | .84 |
| ICU mortality; n (%) | 15 (22) | 31 (19) | .72 |
| Mortality at 28 days; n (%) | 8 (12) | 28 (17) | .32 |
| Mortality at 60 days; n (%) | 13 (19) | 31 (19) | 1 |
DM: diabetes mellitus; HFNO: high flow nasal oxygen; AHT: arterial hypertension; IMV: invasive mechanical ventilation.
The PaO2/FiO2 value upon admission to the ICU was significantly lower in the patients of the first wave (113 [49] versus 157 [74]; P < .05). The use of invasive mechanical ventilation upon admission was also significantly more frequent during the first wave (83% versus 69%; P < .05).
These data are consistent with our working hypothesis, since differences were found in the patient profile and in the therapies used (ventilatory and pharmacological) between the first and the second wave of the COVID-19 pandemic – though no significant differences in ICU mortality were recorded.
A greater number of patients were admitted to intensive care during the second wave, and these individuals were also older, with fewer deaths being recorded. These findings are consistent with those reported by other authors in different countries.7
However, the reasons for these differences between the two periods are not yet clear. In our setting (Spain), it has been postulated that a new SARS-CoV-2 variant appeared early in the summer of 2020, and was associated to outbreaks among young agricultural workers in the north-eastern part of the country. This circumstance, together with poor adherence to the social distancing measures on the part of young people, could have facilitated infection in children and young adults – thereby facilitating the subsequent spread of SARS-CoV-2 to older people more likely to suffer more serious COVID-19.
A study of similar characteristics carried out in France showed that in comparison with the first wave, the second wave was characterized by a lesser proportion of patients requiring invasive mechanical ventilation, and a fewer number of thrombotic events. Likewise, the time between admission to the ICU and tracheal intubation was longer during the second wave, with no significant differences being observed in ICU mortality (50% versus 52%; P = .96) or in the duration of ICU stay.8 However, the mortality rate of the patients requiring mechanical ventilation was 57% versus 75%. Other authors have reported no differences between the two waves in terms of patient age and gender, but found the severity markers to be clearly less prevalent during the second wave, and associated to a 10-fold decrease in mortality rate.9 On the other hand, a Spanish study found that patients admitted to hospital during the second wave were more often treated with noninvasive mechanical ventilation and corticosteroids, and less often with invasive mechanical ventilation, conventional oxygen therapy and anticoagulants – with differences being observed in the mortality risk factors.10
In sum, the present study reveals differences in the therapies used between the two periods, though with no resulting significant differences in terms of mortality. We consider it important to carry out more potent studies to corroborate the true role of the strategies employed in the different waves caused by SARS-CoV-2, and to determine whether these are based on differences in the patient profile.
Conflicts of interestThe authors declare that they have no conflicts of interest in relation to the present study.
Please cite this article as: González-Castro A, Cuenca Fito E, Fernandez A, Escudero Acha P, Rodríguez Borregán JC, Peñasco Y. Primera y segunda oleada de enfermedad por coronavirus-19: un estudio comparativo en pacientes hospitalizados en una UCI de un hospital universitario de tercer nivel. Med Intensiva. 2022;46:166–168.

