





Frailty is a multidimensional syndrome characterized by a deterioration in the functional reserves of various physiological systems. This condition, which is very common in patients admitted to intensive care units (ICUs), results in a state of increased vulnerability, greater care needs upon discharge, and an increased risk of in-hospital mortality and 1 year after discharge.1,2
Frail patients require more resources at the ICU setting. In this regard, frail patients experience longer lengths of stay, a higher need for vasopressors, increased use of mechanical ventilatory support (MVS), and a greater use of renal replacement therapies.3
It is well-known that ICU admissions can have various repercussions including attention and memory disorders, acquired muscle weakness, chronic pain, anxiety, and depression, among others.4,5 However, little is known about the consequences of a serious illness in previously frail patients, both in terms of muscle strength loss and quality of life. Understanding these aspects would allow us to identify the dependency of these patients and plan for social and health care support ate the ICU setting and after discharge.6
The aim of this study was to assess muscle strength and compare quality of life 3 and 9 months after hospital discharge based on the degree of frailty.
A prospective, observational, analytical, single-center study was conducted between November 2018 and July 2019 with ICU survivors from a tertiary hospital who remained hospitalized for, at least, 48 h. Exclusion criteria were: individuals younger than 18 years, neurocritical conditions, and pre-existing cognitive or linguistic disorders hindering communication. The protocol was approved by the corresponding Research Ethics Committee, and prior written informed consent was obtained from the participants.
Patients' frailty prior to ICU admission was determined using the Modified Frailty Index (MFI), which categorizes patients as non-frail, pre-frail, or frail.3,7
Muscle strength at the ICU discharge was assessed using handgrip dynamometry in the dominant hand. Patients underwent early rehabilitation at the ICU. However, after being discharged, there was no such support available in our hospital or at home.
Three and 9 months after ICU discharge, patients were contacted by phone to assess their quality of life using the EuroQol EQ-5D-5L questionnaire.8 To further assess physical functioning, the Patient-Reported Outcomes Measurement Information System (PROMIS v1.2, Physical Function 6b) was used.9
A total of 72 patients were included, and their characteristics are shown in Table 1. Follow-up could not be completed in 6 patients at 3 months and in 11 patients at 9 months due to communication difficulties.
Overall characteristics of the patients.
| Variables | Total(n = 72) | Frail(n = 10) | Pre-frail(n = 27) | Non-frail(n = 35) | P |
|---|---|---|---|---|---|
| Age, years | 51 (33−69) | 70 (62−76) | 60 (48−66) | 39 (26−57) | <.001 |
| Masculine sex | 37 (51%) | 4 (40%) | 12 (44%) | 21 (60%) | .35 |
| Comorbidities | |||||
| AHT | 27 (37%) | 9 (90%) | 18 (67%) | 0 (0%) | <.001 |
| Smoking | 18 (25%) | 3 ()30% | 7 (26%) | 8 (23%) | .89 |
| COPD | 7 (10%) | 3 (30%) | 4 (15%) | 0 (0%) | .01 |
| Heart disease | 12 (17%) | 6 (60%) | 5 (19%) | 1 (3%) | <.001 |
| Diabetes Mellitus | 20 (28%) | 9 (90%) | 11 (41%) | 0 (0%) | <.001 |
| Reason for admission | .39 | ||||
| Infectious | 14 (19%) | 2 (20%) | 5 (19%) | 7 (20%) | |
| Trauma | 13 (18%) | 0 (0%) | 3 (11%) | 10 (29%) | |
| Cardiovascular | 8 (11%) | 1 (10%) | 5 (19%) | 2 (6%) | |
| Respiratory | 9 (13%) | 2 (20%) | 3 (11%) | 4 (12%) | |
| Postoperative | 21 (29%) | 5 (50%) | 8 (30%) | 8 (23%) | |
| Other | 7 (10%) | 0 (0%) | 3 (11%) | 4 (12%) | |
| SAPS 3 | 47.5 (35−54) | 45 (35−50) | 48 (38−54) | 42 (34−58) | .55 |
| Shock | 18 (25%) | 2 (20%) | 7 (26%) | 9 (26%) | .92 |
| MVS | 42 (58%) | 6 (60%) | 18 (67%) | 18 (51%) | .48 |
| Days on MVS | 4 (2−7) | 3 (2−5) | 4.5 (2.5−8) | 5 (2−8.5) | .50 |
| ICU length of stay | 6 (4−13) | 6 (4−11) | 9 (4−15) | 6 (3−14) | .51 |
| Hospital length of stay | 25 (18−44) | 26 (23−51) | 34 (17−54) | 23 (15−38) | .13 |
| 3-month mortality | 11 (15%) | 4 (40%) | 4 (15%) | 3 (9%) | .05 |
| 9-month mortality | 14 (19%) | 4 (40%) | 5 (18%) | 5 (14%) | .19 |
| Dynamometry (Kg) | 22.2 (12.2–32.2) | 13 (11−13) | 19 (12−23) | 26 (21−34) | .003 |
Data are expressed as median (p25−75) or absolute frequency (%).
AHT, arterial hypertension; COPD, chronic obstructive pulmonary disease; ICU, intensive care unit; MVS, mechanical ventilatory support; SAPS 3, Simplified Acute Physiology Score III.
Frailty. A total of 13.9% of the patients (n = 10) met the criteria for frailty (MFI ≥ 3), 37.5% (n = 27) were pre-frail (MFI = 1–2), while the remaining 48.6% (n = 35) fell into the non-frail category. Age was significantly older in frail and pre-frail compared to non-frail patients [70 (62−76), 60 (48−66), and 39 (26−57) respectively; P < .001]. However, SAPS III, the course of MVS, and both the ICU and the hospital lengths of stay were similar, as well as the 3- and 9-month mortality rates across the different frailty categories (Table 1).
Muscle strength. Handgrip dynamometry could be evaluated in 35 patients after the ICU discharge. The strength of frail and pre-frail patients was significantly lower than that of non-frail patients [13(11−13) kg vs 26 (21−34) kg; P = .028; and 19(12−23) kg vs 26 (21−34) kg; P = .015; respectively; Fig. 1A].
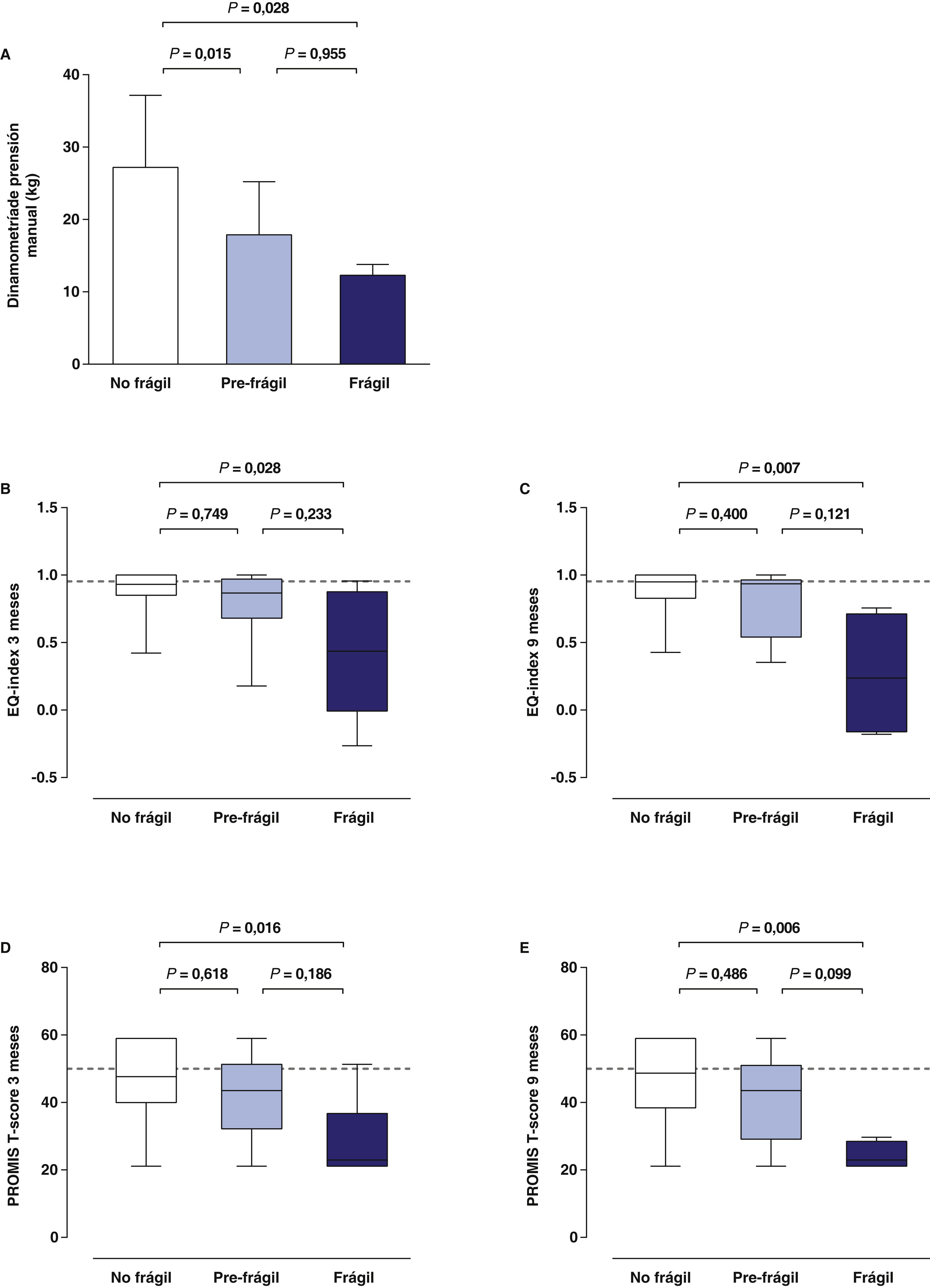
Quality of Life. Quality of life was assessed in 57 patients at 3 months and 43 patients at 9 months (Supplementary Fig. 1). The perceived health status of frail patients was significantly worse than that of non-frail patients, both at 3 [EQ-index 0.43(−0.06−0.8) vs 0.93(0.85–1); P = .028, Fig. 1B], and 9 months [EQ-index 0.23(−0.16−0.71) vs 0.95 (0.82–1); P = .007, Fig. 1C]. The degree of impairment in the 5 dimensions included in the EQ-5D-5 L progressively greater based on the level of frailty, with a negative correlation between the MFI prior to ICU admission and the EQ-index at 3 (Rho = −0.324; P = . 014) and 9 months (Rho = −0.428; P = .004); Supplementary Fig. 1. Both at 3 and 9 months, physical functioning was significantly lower in frail compared to non-frail patients (Fig. 1D and E), with a negative correlation being reported between MFI and Promis (Rho= −0.355; P = .007 and Rho= −0.449; P = .003; at 3 and 9 months, respectively, Supplementary Fig. 1).
Our study identified the negative impact frailty had on strength and quality of life after an ICU experience. Deterioration in these domains is not only due to the degree of critical illness and the therapy received but is also a product of the patient’s pre-existing conditions. The presence of a certain degree of frailty at the ICU admission is associated with worse physical performance and quality of life upon discharge.
Consistent with the above, we found that muscle strength in pre-frail and frail patients decreased at the ICU discharge, maintaining a significantly reduced perception of physical performance compared to other patients for up to 9 months. This raises a scenario of greater dependence on activities of daily living in the long term, adding a high requirement for social and health care support.
Although quality of life at the ICU discharge may be impacted by the severity of illness, the course of MVS, or the ICU length of stay, it is clearly established that pre-existing frailty significantly impacts it.10
Despite our study limitations (single-center with complete follow-up in 60% of the patients, which reduces the statistical power of the results reported), it allowed us to gain insight into relevant aspects of frail patients at the ICU discharge. These aspects should be taken into consideration to establish more accurate prognoses, design adequate therapeutic approaches, and guide the functional expectations of patients and their families.
The following is Supplementary data to this article:


