







To propose a predictive model of secondary traumatic stress (STS).
DesignA descriptive cross-sectional study was carried out.
ContextThe study was conducted in the Intensive Care Units of a hospital in Madrid (Spain).
ParticipantsThe sample comprised 103 health professionals.
InterventionsA series of questionnaires were created and completed by the participants. Network analysis and multiple regression was used for data analysis.
Variables of interestSociodemographic variables such as gender, years of experience and position, STS, passion for work, work stressors, emotional effort, empathy and self-compassion were evaluated.
ResultsThe result identified the following: a) years of experience as a risk factor for compassion fatigue (β=0.224 and P=0.029), and harmonious passion as a protector (β=−0.363 and P=0.001); b) emotional effort and empathy as risk factors for shattered assumptions (β=0.304 and P=0.004; β=0.394 and P=0.000, respectively); and c), work stressors and empathy as risk factors for symptomatology (β=0.189 and P=0.039; β=0.395 and P=0.000, respectively), and years of experience as a protector (β=−0.266 and P=0.002).
ConclusionsThis predictive model of STS identifies protective factors which could be reinforced, such as harmonious passion, and risk factors which should be reduced, such as empathy and emotional effort, with a view to promoting quality of care and quality of life among these professionals.
Proponer un modelo de predictores del estrés traumático secundario (ETS).
DiseñoSe trata de un diseño transversal descriptivo.
ÁmbitoEl estudio se llevó a cabo en las unidades de cuidados intensivos de un hospital terciario de Madrid.
ParticipantesLa muestra estuvo formada por 103 profesionales sanitarios.
IntervencionesSe creó una batería de cuestionarios que fue rellenada por los profesionales. Respecto al análisis de datos, se utilizó una metodología de redes y análisis de regresión jerárquica.
Variables de interésSe evaluaron variables sociodemográficas tales como género, años de experiencia y puesto, el ETS, la pasión por el trabajo, los estresores laborales, el esfuerzo emocional, la empatía, la autocompasión.
ResultadosSe establece: a) para la fatiga por compasión, los años de experiencia como factor de riesgo(β=0,224 y p=0,029), y la pasión armoniosa como protector (β=–0,363 y p=0,001); b) para la sacudida de creencias, el esfuerzo emocional y la empatía como factores de riesgo (β=0,304 y p=0,004; β=0,394 y p=0,000 respectivamente); y c) para la sintomatología, los estresores laborales y la empatía como factores de riesgo (β=0,189 y p=0,039; β=0,395 y p=0,000 respectivamente) y los años de experiencia como protector (β= –0,266 y p=0,002).
ConclusionesEste modelo predictivo del ETS asienta factores protectores que podrían aumentarse, como la pasión armoniosa, y factores de riesgo que sería conveniente reducir, como la empatía y el esfuerzo emocional, con el fin de mejorar la calidad asistencial y de vida de los profesionales.
Intensive care is defined as the field of medicine devoted to managing the critically ill patient. In this setting, numerous studies have provided evidence on the emotional burden of this study where, among other factors, there is a continuous exposure to death, pain, disease, and suffering.1 Also, there are psychosocial risks like exhausting on-call shifts, continuous inflow of patients, need to prioritize the decision-making process under pressure, small working places, and different professionals having to work together.1,2 This working history creates stressors that make it a high-risk job prone to developing certain conditions such as labor disatisfaction, wishes to quit,2 depression, anxiety,3 and burnout syndrome.4–6 On the other hand, and although it has not been studied in this context, it may lead to secondary traumatic stress.7,8
Secondary traumatic stress has been defined as post-traumatic symptoms that may be eexperienced by intensivists, that is, the person who helps the victims of a traumatic event.9 In the intensive care setting, the management of critically ill patients means treating unexpected traumatic, painful events, with the associated emotional burden that means having to cope with the family members who are living moments of crisis.10,11 The study conducted by Domínguez-Gómez and Rutledge12 shows that 33% of the nursing staff that works in the ER setting meet the criteria for secondary traumatic stress.
According to Moreno-Jiménez et al.13 strees leads to 3 different levels of discomfort: (a) compassion fatigue, physical and emotional exhaustion of the healthcare provider; (b) shaken beliefs meaning cognitive changes in beliefs and values in the healthcare provider as a response to the traumatic event lived, and (c) post-traumatic symptoms at cognitive, emotional, and behavioral level as the DSM-V clearly establishes.14 Also, they define empathy and the working history such as time overload or the type of traumatic task as risk factors.9,13 In this study, this history will be referred to as «work-related stressors».
On the other hand, over last few years the studies conducted on burnout syndrome and nursing, confirm the existence of a modifying variable that would be the love for the job.15 The passion for the job has been defined as a «controllable inclination towards an activity that the person values too much and to which he/she decides to devote time and effort».16 There are 2 different types of passion: (a) harmonious passion where the individual controls the activity while in tune with other activities,17 and (b) obsessive passion,18 where the activity controls the person who feels internal or external pressure while trying to achieve certain external contingencies that take on a disproportionate place in his life, creating conflict with other areas.19
Also, both types of passion differ from one another in the associated consequences. In particular, harmonious passion is related to deeper states of concentration (flow for example), life satisfaction, commitment, psychological wellbeing, and positive affectivity,17,20 while obsessive passion is associated with psicological processes like pondering and negative affectivity, role conflict, family-work conflict and burnout syndrome.16,19,21
Finally, there are other emotional variables that may play a significant role in the intensive care setting such as emotional effort and self-compassion. Emotional effort is defined as the discordance experienced by the worker between what he really feels and what he should express in his working environment while interacting with the patients.22 The more common these interactions are the greater the discordance, effort, and emotional exhaustion23 in his working place. Self-compassion, however, is defined as the ability to see defects and errors as a normal part of human condition, which favors the positive relation with oneself and a non-judgemental attitude towards one’s mistakes.24 The studies confirm that when it is high it increases the healthcare providers’ capacity of self-care25 and is associated with a more positive affectivity, psychological health,26 and less stressors of very demanding settings.27
For all this, the goal of this study is to propose a model of secondary traumatic stress predictors to work at an exploratory level. So, for the sake of our model we will be using a job demands and resources (JD-R) model,28 where work-related stressors and emotional effort will be demands associated with the job, while passion for the job, empathy, and self-compassion will be resources of the person capable of favoring or preventing the appearance of secondary traumatic stress.
MethodStudy designThis is a descriptive, transverse study. To achieve maximum efficiency in the evaluation process, the 3 heaviest items in the original confirmatory analysis of the tool were selected for each studied variable. This is the smallest number of items established by statistical models for the representativity of a variable. The weight of an item assesses the degree in which the item measures the construct, which means that the 3 heaviest items were selected. The average time spent to fill out the entire quesionnarie was 15 minunte. The questionnaries used were not validated in the context of an intensive care unit (ICU), but they had been previously validated out-of-hospital emergency settings.
Study variablesThe study variables were sociodemographic variables like genre, age, civil status, working experience, job, working shift, ICU and, finally, whether the staff had had personal traumatic experiences and, if so, which ones.
Questionnaire of Secondary Traumatic Stress.13 This scale includes the assessment of work-related stressors, secondary traumatic stress, and empathy. Regarding these stressors, 4 items from the original scale were included plus 2 items were adapted to the hospital setting («in our unit, time pressure from having to show up where the emergency is occurring is very high» was already present in the original scale and «in our unit, time pressure during early care of the patient is very high» was added as an adapted version. On the other hand, «I find it hard to forget situations where the victim was a minor or an old person» was already included the original scale and the item «the cases somehow similar to my life truly affect me» was also included. Regarding secondary traumatic stress, 3 items were selected for every subdimension. A total of 9 items were collected («I am emotionally overwhelmed by this job», for example). Regarding empathy, the 3 most overwhelming items were selected («I feel a transfer of feelings from my patients», for instance). The response scale was the Likert scale (from 1 to 4), being 1 «totally in disagreement» and 4 «totally in agreement».
The Passion for the Job Scale.29 This scale includes 3 items of harmonious passion (for example, «I live all sorts of experiences with my job») and 3 items of obsessive passion (such as «I emotionally depend on my job»). The response scale was the Likert scale (from 1 to 7), being 1 «totally in disagreement» and 7 «totally in agreement».
The Emotional Effort Scale.30 It includes 3 items such as «during the last month, how often did you feel that this job required great effort?». The response scale went from 1 to 5, being 1 «never» and 5 «always».
The Self-Compassion Scale.26 The 3 most overlwheming items of all from the original short version of 12 items were selected. An example of item here was «I try to see my defects as a normal part of human condition». The response scale was the Likert scale (from 1 to 5), being 1 «rarely» and 5 «almost all the time».
ParticipantsThe study participants were 103 healthcare providers of an intensive care unit from a university tertiary hospital in Madrid, Spain. The study was conducted at the Unit of Intensive Medicine that includes 3 sections: trauma and ER, polyvalent care, and cardiac care unit. The inclusion criteria were being a healthcare provider at an adult ICU with, at least, 2 months of experience. The exclusion criteria were not having spent these 2 months in these ICUs. Before conducting the study, an informative sheet was handed out with the corresponding written informed consent. This project has been approved by the Research Ethics Committee with reference number CEI 71-1276.
Statistical analysisThe statistical analysis was conducted using the SPSS 25.0 software package and included a feasibility analysis of the dimensions of our scale, a descriptive analysis of the variables of interest, a MANOVA analysis to study possible differences of genre, ICU and position in the variables of interest. Finally, one logistics regression analysis using as criterion variables the 3 separate subdimensions of secondary traumatic stress: shaken beliefs, fatigue due to compassion, and traumatic symptoms.
On the other hand, a network model known as «psychological network» was designed.31 The JASP32 statistical software package was used. This software builds an interface for R through which this type of model is generated. This model is used to analyze the most significant estimators: strength, nearness and interconnectivity.31 The order from less to greater complexity is: 1) «strength», meaning the total intensity with which a variable is related to the network measured as the sum of all links different than zero; 2) «nearness», meaning the tendency of a variable to be connected to others (being «near») measured as the number of connections other than zero in every variable; and 3) «interconnectivity», meaning the tendency of a variable to mediate between 2 and measured as the number of pairs other than zero of a variable with 2 different variables. Therefore, a variable with high strength implies that, regardless of how it is distributed, it intensely connects to the rest of the network through a single very intense link, several not so intense links or intermediate links. Variables with high nearness mean they are connected to many other variables in the network. High interconnectivity means that other 2 variables can connect to one another. If a variable has high strength, nearness, and interconnectivity, that means it is a fairly central variable within the network, both numeric and graphically, that it connects to many other variables with intensity, and that it interconnects several variables to one another. To interpret these indicators on Fig. 1, positive values indicate values above average and the negative ones indicate values below average.
Results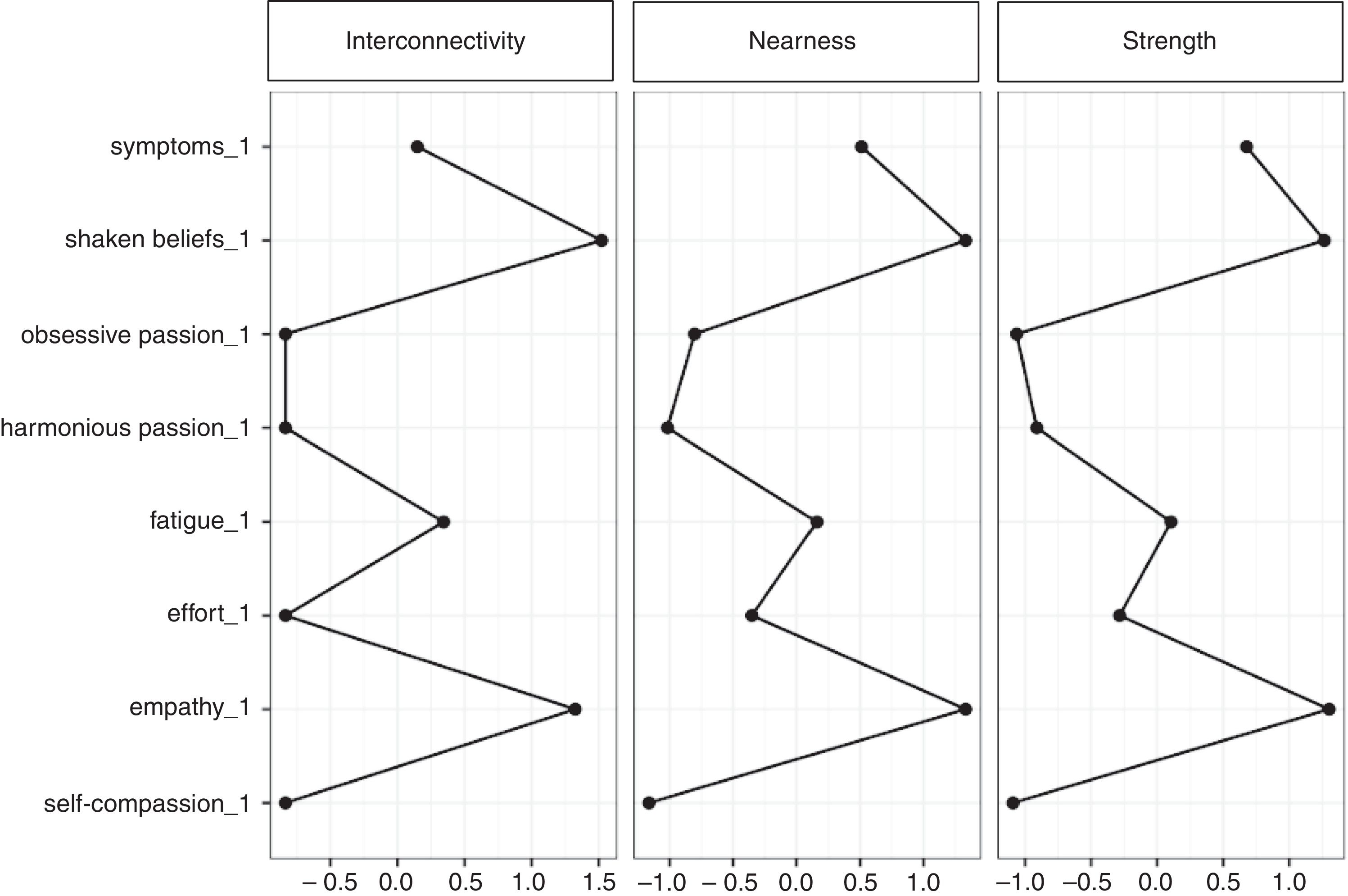
The total study sample consisted of 103 patients including 36 males (35.3%) and 66 women (64.7%). The mean age was 37.23 years (TD=11.47) ranging between 21 and 64 years. Also, 71.8% of the study sample said they were in a stable relation, as opposed to 18%, and 8% who said they were not involved in a sentimental relation. The experience of the sample in the healthcare setting was 13.62 years on average (TD =9.22). Participants included 35 doctors, 49 nurses, 16 assistants, and 2 porters. Also, a distinction was made on an ICU basis: a sample of 35 staff members working at trauma and ER ICUs was selected: 39 from coronary ICUs and 25 from polyvalent ICUs. Another 3 participants said they worked in these 3 units. Seventy-six participants worked during the morning shift, 16 during the afternoon shift, 5 participants during both shifts, while only 1 reamained on call. On ther other hand, 65% of the sample said they had not had direct personal traumatic experiences before.
Table 1 shows the means expressed as the average of the scores obtained for each scale and the main correlations of our variables of interest. No significant differences were seen when differences in the variables of interest based on genre, position, and ICU were analyzed.
Means, typical deviations, and bivariate correlations in the study variables.
| Variables | M | TD | α | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Work-related stressor | 3.02 | 0.34 | 0.63 | 1 | ||||||||
| Emotional effort | 2.88 | 0.75 | 0.72 | 0.35** | 1 | |||||||
| Fatigue due to compassion | 1.83 | 0.45 | 0.58 | 0.16 | 0.27** | 1 | ||||||
| Shaken beliefs | 2.96 | 1.36 | 0.71 | 0.31** | 0.46** | 0.47** | 1 | |||||
| Symptoms | 2.20 | 0.49 | 0.81 | 0.41** | 0.33** | 0.136 | 0.37** | 1 | ||||
| Harmonious passion | 3.28 | 0.86 | 0.49 | −0.08 | −0.23** | −0.39** | −0.15 | 0.61 | 1 | |||
| Obsessive passion | 2.88 | 0.75 | 0.74 | 0.15 | 0.01 | 0.13 | 0.09 | 0.17 | −0.03 | 1 | ||
| Empathy | 2.20 | 0.49 | 0.69 | 0.38** | 0.324** | 0.21* | 0.50** | 0.58** | 0.02 | 0.33** | 1 | |
| Self-compassion | 3.28 | 0.87 | 0.68 | −0.13 | −0.16 | −0.08 | −0.13 | −0.31** | 0.129 | −0.25** | −0.23 | 1 |
α=Cronbach’s alpha for the variables of interst; M, mean; TD, typical deviation.
Fig. 2 shows the final network model with the significant correlations. We can see that self-compassion keeps a negative correlation with obsessive passion and symptoms, meaning that it would be a protective factor. The same thing happens with harmonious passion that keeps a negative correlation with shaken beliefs and symptoms. On the other hand, empathy and emotional effort are risk factors that keep a with positive correlation with symptoms and shaken beliefs unlike harmonious passion.
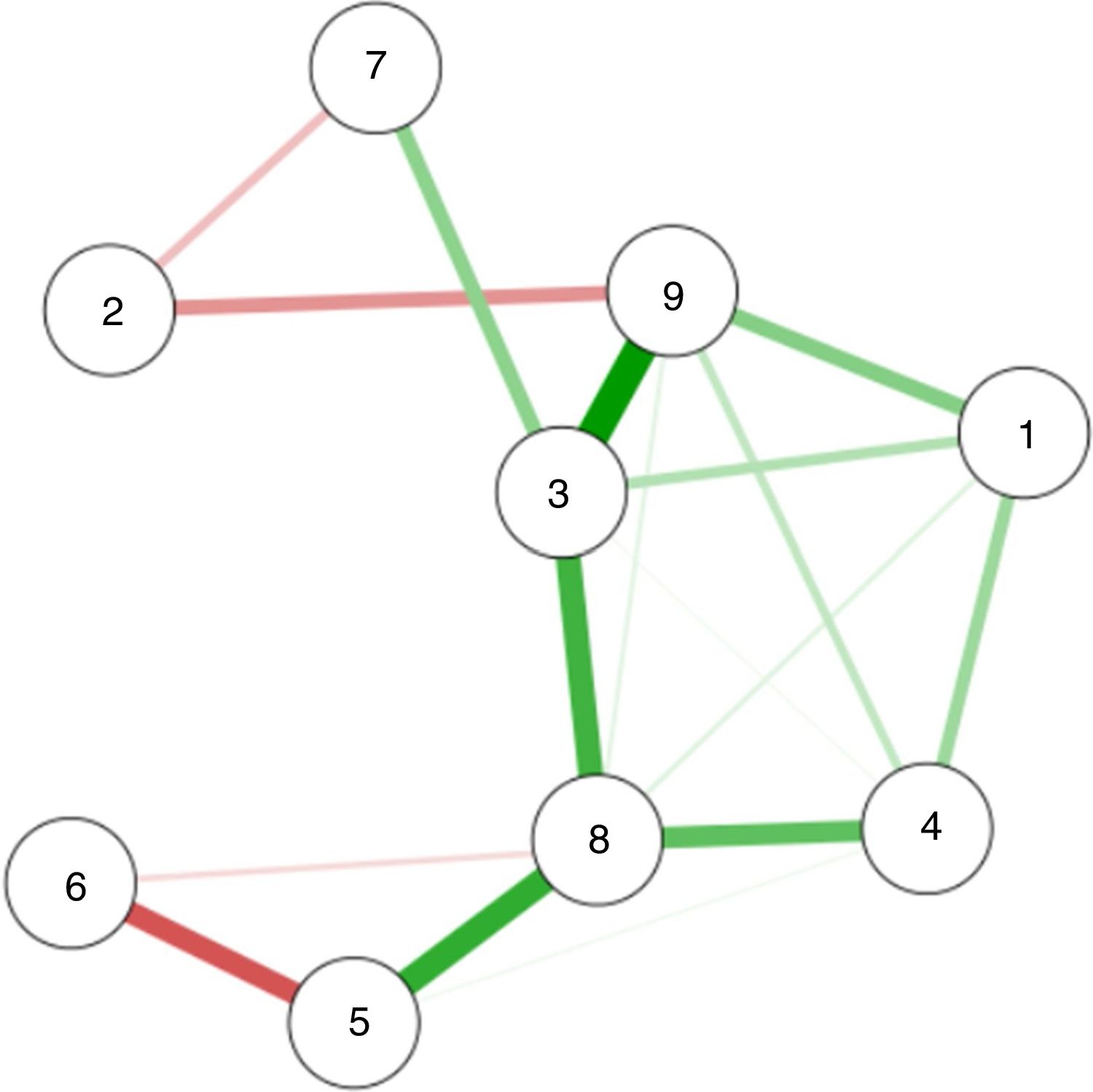
Network model with significant correlations of the variables of interest. Thickness: it indicates the intensity of the association. Greater thickness, greater intensity; less thickness, less intensity.
Green color: positive correlations; pink color: negative correlations.
1: work-related stressors; 2: self-compassion; 3: empathy; 4: emotional effort; 5: fatigue due to compassion; 6: harmonious passion; 7: obsessive passion; 8: shaken beliefs; 9: traumatic symptoms.
Fig. 1 shows centrality estimation. The 2 most significant variables in the 3 estimators that are above the rest are shaken beliefs («shaken beliefs_1») and empathy («empathy_1»). This points to both variables as especially significant within the network. On the other hand, traumatic symptoms («symptoms_1») and fatigue due to compassion («fatigue_1») are the next most significant variables with mean centrality. Together with the network, these results provide information on this possible variable core by interconnecting parts of the network with more peripheral parts. In particular, both self-compassion and harmonious passion seem to be more peripheral to the network and keep negative correlations to the rest; that is, they are protective while the remaining variables often keep a positive correlation to one another.
Multiple regression analysisTable 2 shows regressions of the different dimensions of secondary traumatic stress. This table shows the values of variance explained for each of the 3 models. The model of symptom variance is the one that presents the greater percentage of variance explained (45%) with significant increases as sociodemographic, work-related stressor, emotional effort, empathy and self-compassion variables were being added to the model.
Multiple hierarchical regression for the dimensions of secondary traumatic stress.
| Steps of the model and variables | Fatigue due to compassion | Shaken beliefs | Traumatic symptoms | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pending (β) | Pending (β) | Pending (β) | ||||||||||
| Step#1 | ||||||||||||
| Genre | 0.218* | 0.182 | 0.170 | 0.160 | 0.171 | 0.075 | 0.072 | 0.042 | 0.055 | −0.047 | −0.027 | −0.043 |
| Position | −0.023 | −0.027 | −0.021 | −0.013 | −0.029 | −0.001 | 0.000 | 0.025 | −0.252** | −0.206* | −0.183 | −0.161 |
| Years of experience | 0.149 | 0.196 | 0.207 | 0.224* | −0.025 | 0.044 | 0.046 | 0.085 | −0.368** | −0.336** | −0.338** | −0.266** |
| Step#2 | ||||||||||||
| Work-related stressors | −0.010 | −0.020 | −0.050 | 0.175 | 0.173 | 0.093 | 0.298** | 0.282** | 0.189* | |||
| Emotional effort | 0.066** | 0.230* | 0.191 | 0.417** | 406*** | 0.304** | 0.189 | 0.218** | 0.099 | |||
| Step#3 | ||||||||||||
| Harmonious passion | −0.343** | −0.363** | −0.058 | −0.119 | 0.135 | 0.094 | ||||||
| Obsessive passion | 0.130 | 0.092 | 0.020 | −0.078 | 0.077 | −0.057 | ||||||
| Step#4 | ||||||||||||
| Empathy | 0.141 | 0.394** | 0.395** | |||||||||
| Self-compassion | −0.008 | 0.28 | −0.150 | |||||||||
| Adjusted R2 | 0.200 | 0.314 | 0.450 | |||||||||
| ΔR2 | 0.056 | 0.083* | 0.128** | 0.014 | 0.030 | 0.241** | 0.004 | 0.109** | 0.191*** | 0.153*** | 0.022 | 0.139** |
Standardized β values and level of significance.
Adjusted R2: percentage of variance explained with the inclusion of the variable.
When analyzing the beta values standardized on Table 2, we should be looking at the last column of every dimension of secondary traumatic stress referring to the final step of regression. Regarding the first component of secondary traumatic stress—the variable fatigue due to compassion—only the years of experience proved to be a positive predictor of the variable, while harmonious passion appears as a negative predictor.
Regarding the second component—shaken beliefs—both emotional effort and empathy are positive predictors. This may explain the results of Table 1 where both variables keep significant and positive correlations.
If we analyze the third component—traumatic symptoms—we will find the years of experience again but, in this case, as a negative predictor, while work-related stressors and empathy appear as positive predictors.
DiscussionThis study tried to establish a model of significant predictors for secondary traumatic stress obtaining similar information from the network model and the regression analysis.
Regarding fatigue due to compassion—wear and tear due to empathy from the healthcare provider—harmonious passion acts as a protector, which is indicative that the more balanced a person is in the different areas of his life (work, family, friends, etc.) the less his wear and tear conflict will be in his job. It can also favor further experiences of recovery and disconnection,15 more self-care, and less fatigue due to compassion. On the other hand, the years of experience in this sector are a risk factor in this dimension, which would not be consistent with with prior studies.33 These results are indicative that this dimension would be associated with the degree of exposure to trauma since longer times of exposure by the professional equal greater wear and tear.
Regarding shaken beliefs, both empathy and emotional effort are risk factors indicative that the greater the capacity of the healthcare provider to understand the emotions of patients and their families and the greater his effort the more changes in values and beliefs. These results are consistent with former studies where they have been proposed as risk factors.2,9,13,22 Also, gathering qualitative evidence through interviews with the healthcare providers is indicative that, on many occasions, they are aware of cognitive changes in their values and beliefs due to their job (for example, car crashes with young people involved, spinal cord injuries, etc.), but they are not aware of the emotional impact. For this reason, the shaken beliefs variable can have greater specific weight in this setting,34 as the network model showed.
Also, regarding symptoms, the years of experience are a protective factor that is consistent with what the scientific references tell us.33 The explanation may be that the more exposed healthcare providers are to their job, the less evident their symptoms become. Another alternative may be the parallel development of protective variables as the personnel gains experience (like self-compassion),27 favoring more self-care initiatives and protection from the most psychosomatic features of secondary traumatic stress. On the other hand, regarding the risk factors for post-traumatic symptoms, work-related stressors play an important role here, which would make sense from a theoretical point of view since longer exposure to these stressors lead to more symptoms.13 Again empathy is a tool for people with negative consequences.9,13
Lastly, obsessive passion appears in the network model as a risk factor for empathy, symptoms, and shaken beliefs. As Donahue et al.15 say these results would be relevant if greater obsessive passion were associated with greater processes of pondering and less recovery which would favor the appearance of more symptoms by reviving the discomfort experienced during the working day and never getting a break. Also, the conflict generated by other vital areas18 may cause greater changes in the workers’ beliefs by letting these traumatic situations have a greater impact in their lives. On the other hand, this passion promotes empathy which is, in turn, a risk factor. We can say that the most obsessive part of passion that «urges» workers to keep on working would have to do with the mechanisms that make a person empathetic to patients and families and facilitate counter-productive emotional contagion. These results would be different from those of other studies where empathy is associated with less burnout syndrome35 and more wellbeing.36
Regarding the limitations of this study, its transversal methodology makes it difficult to establish causal relations, meaning that it is necessary to develop a longitudinal study to establish the models of mediation and moderation of the study variables. Another limitation has to do with the intensive care setting per se, since the flow of patients and changes of activity make it difficult to gather information and respond to the corresponding scales. To mitigate this stressor the number of items in the assessment questionnaire was reduced to avoid saturating the workers. This led to another limitation: the poor reliability of certain items, which made us eliminate a few variables that were initially part of the study. Added to this control a statistical analysis of realiability was conducted in each variable by eliminating an element to select the most reliable items for measuring purposes and, eventually, ameliorate this limitation. This setting is also the origin of another limitation: the small size of sample and center that is an actual threat to the study external validity. However, obtained significant preliminary results for future replicas in other centers.
ConclusionsIn conclusion, our study is the first one on secondary traumatic stress in the healthcare population of intensive care units. From the data obtained we can go deep into the measures aimed at improving the quality of life of these professionals and impacting the quality of the healthcare provided.37,38 For all this, it is crucial to propose intervention designs to prevent secondary traumatic stress, reduce the risk factors found in this study such as empathy and emotional effort, and increase protective factors like self-compassion and harmonious passion.
FundingThese have been the sources of funding for this project:
Predoctoral contract FPI-UAM 2017 of the Universidad Autónoma de Madrid and project PSI2015-68011-R of the Spanish Ministry of Economy and Competitivity (MINECO).
Authors/CollaboratorsAll authors participated in the design, analysis, and development of this study. In particular, Mario Chico, Marisol Martínez, and Juan Carlos Montejo participated in the study design and facilitated data mining at the hospital and adapted the measuring tool to their hospital setting. On the other hand, Raquel Rodríguez-Carvajal and Bernardo Moreno-Jiménez participated in the design and creation of the measuring tool and its applicability. They also participated in the discussion of the results and implementation in future studis. Óscar Lecuona also participated in the design, methodology, and data analysis. Finally, Eva Garrosa directed the applicability study at the hospital and the study.
Conflict of interestsNone reported.
We wish to thank the Intensive Care Units of the Hospital Doce de Octubre, Madrid, Spain and, in particular, the entire healthcare personnel that participated and always trusted this project.
The following is Supplementary data to this article:

Please cite this article as: Moreno-Jiménez JE, Rodríguez-Carvajal R, Chico-Fernández M, Lecuona Ó, Martínez M, Moreno-Jiménez B, et al. Factores de riesgo y protección del estrés traumático secundario en los cuidados intensivos: un estudio exploratorio en un hospital terciario de Madrid. Med Intensiva. 2020;44:420–428.

