

To stay in an intensive care unit (ICU) is an experience that has a tremendous impact on the quality of life of the patients.1 In several interviews, an important politician in Spain has expressed the pain and fear suffered during her ICU stay, which she described as the ‘vestibule of hell’. This perception has not left indifferent the professionals that we devote ourselves to the intensive care.
Patients in critical condition who are admitted to our units often find themselves immersed in a plethora of cables and sophisticated monitoring and life-support equipment. When the medical priority is to provide diagnostic support and treatment urgently needed, this tends to produce a kind of depersonalization of the patient. Nevertheless, the patients, at some point, become aware of their surroundings and later they are able to recall them.2
The consequences of life-support for those who survive an ICU stay invite reflection on certain aspects of this question which have, to date, been relegated to the background.3,4 The main concern in intensive care medicine, from an ethical perspective, has been to insure that the life support provided to each patient is consistent with that patient's needs so as to avoid therapeutic obstinacy, as well as to be able to detect and attend to end-of-life situations in an appropriate manner. This, in terms of principle-based bioethics, would correspond to non-malfeasance or beneficence.5 Also requiring reflection is the autonomy of the critically ill patients, given that they may not be in any condition to competently make decisions; in the absence of a living will, consent is required of a representative, either a family member or legal counsel.6
Patient testimonials or initiatives such as the HU-CI blog,7 highlight the fact that the principalist bioethics does not respond to all situations that can cause suffering to the people admitted to the ICU, so new ethical view is necessary; this time to try to modify the operation of the UCI and the attitude of the professionals, in order to reduce as much as possible the fear and pain, besides its consequences. Bioethical principles and code of the Spanish Society of Intensive Care Medicine (SEMICYUC) can help, but it is imperative a broader perspective.8
Care ethics could be defined as a type of relational ethics that ensures autonomy of vulnerable persons and uses a relational and context-bound approach toward morality and decision making.
Autonomy, in this case, is understood in a context, not self-sufficiency or independence, but interdependence. We live in a social framework which we need to be ourselves, to make our own decisions. The autonomy to which we refer is the moral ability to direct our own lives.9,10
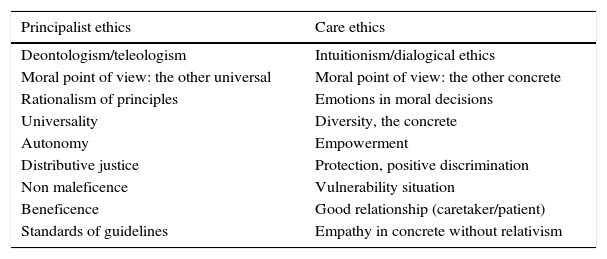
The ethics of care retrieves the affective and emotional supplementing a bioethics more rational as based on principles (Table 1).11 This can influence to improve the experience of patients in the ICU, putting it in the foreground, in the center of attention. In a study that showed that admission to the ICU of patients with a limitation in life-support treatment was a common practice, Rubio noted that decision-making on the futility of a treatment is an act with ethical and moral implications.12 This alludes to the ethics of accountability—a necessary virtue for the professional who has to assume the responsibility for this decision-making. To respond is to take charge, to look after and care for a fragile individual. The ethics of care touch upon the emotional and affective domains which may have a part to play in improving the experience of patients in the ICU, placing this question at the heart of the matter. It is, of course, fundamental to include the physician in the task of caring, without restricting the work of nurses, as has been the case till now. Care should not be encumbered by professional or jurisdictional barriers.
The ethics of care retrieves the affective and emotional supplementing a bioethics more rational as based on principles.
| Principalist ethics | Care ethics |
|---|---|
| Deontologism/teleologism | Intuitionism/dialogical ethics |
| Moral point of view: the other universal | Moral point of view: the other concrete |
| Rationalism of principles | Emotions in moral decisions |
| Universality | Diversity, the concrete |
| Autonomy | Empowerment |
| Distributive justice | Protection, positive discrimination |
| Non maleficence | Vulnerability situation |
| Beneficence | Good relationship (caretaker/patient) |
| Standards of guidelines | Empathy in concrete without relativism |
One conclusion of a study entitled ‘Sufrimiento y su afrontamiento en la UCI’ (Facing Suffering in the ICU)13 is that the strategies for facing suffering, on both parts, patients and their families, were based on medical information (in addition to family support). The fact that nursing carries care as a virtue does not mean that the physician should not provide more than technical expertise, clinical practice guides, and protocols.
These strategies are necessary for the care, but they are not enough to reveal the person that may be found in the patient who is under care. Care requires a reciprocal relationship; if the carer does not identify what makes the patient different from all others, then to attend that patient's real needs will be nearly impossible. It is of the utmost importance to focus diagnostic and therapeutic strategies attentively toward the singularity of each patient; we are not there, after all, to treat illnesses, but rather people who are ill.
We all, as humans, require care at one time or another in our lives in order to develop as people, so that our voice, which makes each of us unique, may be heard. Caring and being cared for are indispensable parts of our survival, and those in the ICU finds themselves in a situation of great vulnerability in many ways. Levinas maintains that attending the Other (a term he uses to refer to a human being that is suffering) is a moral imperative, an inescapable call.14 When care is professionalized, it acquires a normative dimension. Healthcare personnel take on a moral commitment to others; care is the internal goods of the healthcare profession and a desirable virtue in those working in the ICU. In order to establish the relationship of care, the carer, as a professional, must take on among other virtues compassion and concern for the well-being of the patient. But even this is not enough, if it is not accompanied by action, by an attentive gaze, and by the application of technical know-how. Ethical care allows for an understanding of a person's needs beyond the purely biological in order to assume control over physical and psychological pain.
New ethical points of views are necessary to humanize intensive care, and physician involvement is essential in this process. Care ethics is a fundamental foundation for the building of the friendly ICU that we are starting to conceive of, an ICU in which patients and their families are treated well and recognize this. From this point, admission to the ICU can stop being a prelude to horrors.
FundingThe preparation of this manuscript has not sought nor received funding.
Conflict ofinterestThere has been no conflict of interest in the preparation of this manuscript.

