






To determine factors related to limitations on life support within 48h of intensive care unit (ICU) admission.
Study designProspective multicenter study.
SettingEleven ICUs.
PatientsAll patients who died and/or had limitations on life support after ICU admission during a four-month period.
VariablesPatient characteristics, hospital characteristics, characteristics of limitations on life support. Time-to-first-limitation was classified as early (<48h of admission) or late (≥48h). We performed univariate, multivariate analyses and CHAID (chi-square automatic interaction detection) analysis of variables associated with limitation of life support within 48h of ICU admission.
Results3335 patients were admitted; 326 (9.8%) had limitations on life support. A total of 344 patients died; 247 (71.8%) had limitations on life support (range among centers, 58.6%–84.2%). The median (p25–p75) time from admission to initial limitation was 2 (0–7) days. CHAID analysis found that the modified Rankin score was the variable most closely related with early limitations. Among patients with Rankin >2, early limitations were implemented in 71.7% (OR=2.5; 95% CI: 1.5–4.4) and lung disease was the variable most strongly associated with early limitations (OR=12.29; 95% CI: 1.63–255.91). Among patients with Rankin ≤2, 48.8% had early limitations; patients admitted after emergency surgery had the highest rate of early limitations (66.7%; OR=2.4; 95% CI: 1.1–5.5).
ConclusionLimitations on life support are common, but the practice varies. Quality of life has the greatest impact on decisions to limit life support within 48h of admission.
Determinar los factores relacionados con la limitación del tratamiento de soporte vital (LTSV) en las primeras 48h de ingreso en Unidades de Cuidados Intensivos (UCI).
DiseñoMulticéntrico prospectivo.
ÁmbitoOnce UCI.
PacientesPacientes fallecidos y/o en los que se aplicó LTSV durante 4 meses.
Variables de interésCaracterísticas de pacientes, hospital y LTSV. Se definió LTSV precoz la que ocurría en las primeras 48h de ingreso y tardía >48h. Realizamos análisis univariado, multivariado y árbol de decisión chi-square automatic interaction detection (CHAID) con las variables asociadas con LTSV en las primeras 48h.
ResultadosIncluidos 3.335 pacientes, en 326 (9,8%) se aplicó LTSV y 344 fallecieron; de estos 247 (71,8%) se limitaron (variabilidad interhospitalaria: 58,6-84,2%). La mediana de tiempo (p25-p75) entre el ingreso y la LTSV inicial fue de 2 (0-7) días. El análisis CHAID evidenció que la escala de Rankin modificada fue la variable más estrechamente relacionada con la limitación precoz. Entre los pacientes con Rankin>2 la LTSV precoz se realizó en el 71,7% (OR=2,5; IC 95%: 1,5-4,4) y la enfermedad pulmonar fue la variable más relacionada con la LTSV precoz (OR=12,29; IC 95%: 1,63-255,91). Entre los pacientes con Rankin≤2, la LTSV precoz ocurrió en el 48,8% siendo los pacientes con cirugía urgente aquellos con mayor LTSV precoz (66,7%; OR=2,4; IC 95%: 1,1-5,5).
ConclusiónLa LTSV es común pero la práctica es variable. La calidad de vida es la variable que mayor impacto tiene sobre la LTSV en las primeras 48h del ingreso en la UCI.
In critical patients, end-of-life decisions, especially the decision to limit life support, are controversial,1 although there is a clear consensus that a terminal patient's life should not be prolonged unnecessarily.2–5 The European Medical Ethics Code recommends that physicians should implement appropriate measures to achieve patient well-being, while avoiding futile, unnecessary, or ineffective diagnostic or therapeutic measures with no hope of benefits.6 Predicting prognosis is important for end-of-life decisions, and various systems based on severity scores have been developed for this purpose. However, as Le Gall points out, although good severity systems can accurately estimate the number of patients that will die in groups of similar patients, they cannot predict which patients will die.7
Publications in the last two decades show life support is often limited in ICUs.8,9 Limitations on life support vary with multiple cultural, religious, organizational, and politicolegal factors.8 Scant information is available about factors related with the timing of orders to limit life support. The primary objective of this study was to determine which factors are related to limiting life support within 48h of ICU admission. Secondary objectives were to determine which variables influence end-of-life decisions and the types of limits on life support in our environment.
Patients and methodsDesign, setting and participating centersThis prospective, observational and open study included all patients admitted to the ICU who died or had any limitations on life support in 11 Spanish ICUs from 1 March through 30 June 2013. At each participating center, a researcher extracted information about end-of-life care and limitations on life support from clinical sessions and medical records.
The clinical research ethics committees at all participating centers approved the study and waived the requirement for informed consent because no interventions were done. Table 1e reports the characteristics of participating centers [see electronic supplementary material (ESM)].
Study variablesWe recorded demographic characteristics (age and sex), toxic habits, pre-ICU quality of life (modified Rankin scale10,11), and comorbidities (hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), liver disease, heart disease, active cancer, or cancer in complete remission). We classified patients according to type (medical, surgical, or trauma), diagnostic category (cardiovascular, pulmonary, infectious, neurological, metabolic, gastrointestinal, or cardiopulmonary arrest), and chronicity (acute or acute-on-chronic). We classified centers according to level of complexity, physicians’ experience, and whether they had transplant and/or organ donor programs. In all patients, the surgical decision was determined only by surgeons
Limitations on life support: definitionsLife-support measures considered were vasoactive drugs, mechanical ventilation, continuous renal replacement techniques (CRRT), antibiotics, transfusion of blood products, and enteral and/or parenteral hydration and nutrition.12 No general protocol to limit life-support measures was applied. Attending physicians were responsible for deciding whether to apply life-support measures; decisions were reached in conjunction with the multidisciplinary team according to local protocols fulfilling the Spanish Society of Critical Care Medicine's (SEMICYUC) recommendations.4
Limitation of life support was defined as withholding or withdrawing one or more life-support measures. Do-not-resuscitate orders and conditioned intensive therapy were considered specific modalities of limitations on life support. We excluded patients admitted for nontherapeutic elective ventilation. We analyzed the time from admission to the first decision to limit life support, the life-support measure limited, the modality of limitation (withdrawing, withholding, do-no-resuscitate orders, or conditioned intensive therapy), and the reasons justifying this decision (age; functional disability; diagnostic category; multiple organ failure; or therapeutic futility, defined as failure of a treatment to accomplish its intended physiological goal).
We classified the time when the decision to limit life support was made as early (<48h from ICU admission) or late (≥48h after admission). We did not analyze the subgroup of patients with limitations on life support upon ICU admission.13
We recorded whether the medical team, nursing staff, and family members participated in end-of-life care and decisions, as well as whether the patient's wishes were expressed in an advance life directive.
When more than one decision to limit life support was registered, the one registered at the latest time was considered the last one; if only one decision was registered, it was considered the first and last one. All patients included in the study were monitored until discharged from hospital.
Statistical analysisDiscrete variables are expressed as frequencies (percentages), and continuous variables as means and (standard deviations) or medians (p25–p75). Differences in demographic and clinical characteristics between groups were assessed with chi-square tests or Fisher's exact test for categorical variables and with Student's t-test or the Mann–Whitney U test for continuous and ordinal variables, as appropriate. Significance was set at p<0.05. We used chi-square automatic interaction detection (CHAID) analysis to elaborate a decision tree (graphic representation of a set of decision rules)14,15 to determine the profile of patients most strongly associated with early decisions to limit life support. We constructed a multivariable logistic model in which the dependent variable was early decision to limit life support and the independent variables were all those significant in univariate analyses and those considered clinically relevant at ICU admission (age, Rankin scale, COPD), patient type (medical, surgical, trauma), diagnostic category (pulmonary or neurological); and characteristics of the centers and staff (staff experience, availability of a protocol for limitations on life support, presence of a transplant program, and organ and tissue donation activity). We used SPSS 22.0® for all analyses.
ResultsDuring the study period, 3335 patients were admitted; life support was limited in 326 (9.8%). A total of 344 patients died; life support was limited in 247 (71.8%) of these. The percentage of patients who died after life support was limited varied widely among centers (58.6%–84.2%). Table 1 summarizes the characteristics of patients in whom life support was limited. The median age of patients with limitations on life support was 75 (65–80) years; 207 (63.5%) were men. Limitations on life support were more common in patients with acute medical conditions and in those with neurological disease. The first limitation consisted of withholding life support measures in 70.9% and of withdrawing measures in 22.7%. Conditioned intensive therapy was implemented in 6 (1.8%) patients, and do-not-resuscitate orders in 15 (4.6%); life-support measures were eventually withdrawn in more than 50% of the patients in these two groups.
Characteristics of patients with limitations on life support.
| Patients with some type of limitation on life support (n=326) | ||
|---|---|---|
| Age, median (p25–p75) | 75 (65–80) | |
| APACHE II, median (p25–p75) (n=260) | 21 (17–26) | |
| SAPS II, median (p25–p75) (n=161) | 48 (37.5–60.5) | |
| Modified Rankin Scale, median (p25–p75) | 2 (0–3) | |
| Days from admissions to limitation, median (p25–p75) | 2 (0–7) | |
| Men, n (%) | 207 | 63.5 |
| Intensive care unit mortality, n (%) | 217 | 66.6 |
| Hospital mortality, n (%) | 247 | 75.8 |
| Comorbidities | ||
| Smoking, n (%) | 54 | 6.6 |
| Alcohol, n (%) | 36 | 11 |
| Hypertension, n (%) | 196 | 60.1 |
| Chronic obstructive pulmonary disease, n (%) | 113 | 34.7 |
| Diabetes mellitus, n (%) | 99 | 34.4 |
| Chronic kidney disease, n (%) | 49 | 15.0 |
| Liver disease, n (%) | 40 | 12.3 |
| Cardiovascular disease, n (%) | 123 | 37.7 |
| Active cancer, n (%) | 66 | 20.2 |
| Cancer in complete remission, n (%) | 22 | 6.7 |
| Type of disease | ||
| Acute disease, n (%) | 242 | 74.2 |
| Acute-on-chronic disease, n (%) | 84 | 25.8 |
| Patient type | ||
| Medical, n (%) | 234 | 71.8 |
| Trauma, n (%) | 15 | 4.6 |
| Emergency surgery, n (%) | 54 | 16.6 |
| Scheduled surgery, n (%) | 23 | 7.1 |
| Diagnostic category | ||
| Cardiovascular, n (%) | 47 | 14.4 |
| Pulmonary, n (%) | 47 | 14.4 |
| Infectious, n (%) | 63 | 19.3 |
| Metabolic, n (%) | 5 | 1.5 |
| Gastrointestinal, n (%) | 41 | 12.6 |
| Neurological, n (%) | 70 | 21.5 |
| Cardiorespiratory arrest, n (%) | 40 | 12.3 |
| Life support measures limited | ||
| Vasoactive drugs, n (%) | 196 | 60.1 |
| Invasive mechanical ventilation, n (%) | 268 | 82.2 |
| Noninvasive mechanical ventilation, n (%) | 61 | 18.7 |
| Continuous renal replacement techniques, n (%) | 44 | 13.5 |
| Reason for life support treatment limitationa | ||
| Age, n (%) | 79 | 24.2 |
| Degree of functional disability, n (%) | 68 | 20.9 |
| Comorbidities, n (%) | 157 | 48.2 |
| Reason for admission, n (%) | 185 | 56.7 |
| Therapeutic futility, n (%) | 190 | 58.6 |
| Multiorgan failure, n (%) | 83 | 25.5 |
| Others, n (%) | 34 | 10.4 |
Abbreviations: APACHE: Acute Physiologic and Chronic Health Evaluation; SAPS: Simplified Acute Physiology Score.
The life-support measures most often withheld were mechanical ventilation (45.7%), vasoactive drugs (37.7%), and CRRT (37.4%). The life-support measures most often withdrawn were mechanical ventilation, withdrawn in 49 (15%) patients, including extubation in 18 (5.5%), followed by vasoactive drugs, withdrawn in 38 (11.7%) patients (Table 2).
Type of life support treatment limitation.
| Type of life support treatment limitation | n | % |
|---|---|---|
| Conditioned intensive therapy,n(%) | 6 | 1.8 |
| Do not resuscitate order,n(%) | 15 | 4.6 |
| Withholding of measures,n(%) | 231 | 70.9 |
| Vasoactive drugs | 123 | 37.7 |
| Invasive mechanical ventilation | 149 | 45.7 |
| No orotracheal intubation | 104 | 31.9 |
| No increase FiO2 | 45 | 13.8 |
| No invasive mechanical ventilation | 4 | 1.2 |
| No continuous renal replacement techniques | 122 | 37.4 |
| No antibiotic | 5 | 1.5 |
| No surgery | 54 | 16.6 |
| No transfusion | 17 | 5.2 |
| No hydration/nutrition | 2 | 0.6 |
| Withdrawal of measures,n(%) | 74 | 22.7 |
| Drugs vasoactive | 38 | 11.7 |
| Invasive mechanical ventilation | 49 | 15 |
| Decrease FiO2 | 25 | 7.7 |
| Extubation | 18 | 5.5 |
| Terminal weaning | 5 | 1.5 |
| Hypoventilation | 8 | 2.5 |
| No invasive mechanical ventilation | 2 | 0.6 |
| Continuous renal replacement techniques | 11 | 3.4 |
| Antibiotic | 4 | 1.2 |
| Hydration/nutrition | 2 | 0.6 |
Abbreviations: FiO2: fraction of inspired oxygen.
The most common reason for the first limitation of life support was therapeutic futility, used to justify the decision in 190 (58.6%) cases; the least frequent reasons were degree of functional disability, cited in 68 (20.9%) cases, and age, cited in 79 (24.2%) (Table 1).
The medical team reached a consensus about the decision to limit life support in 97.2% of cases. The nursing team participated in 57.1%, and family members agreed with the decision in 84%. The decision to limit life support was recorded in the medical history in 82.2% of cases, and only 5.2% of patients had advanced life directives.
In 72 (22%) patients, more than one decision to limit life support was taken, although the percentage of patients with more than one decision varied widely among centers (4.4%–41.2%). Compared with the first decision, a larger percentage of the last decisions to limit life support were to withdraw life-support measures (77.7% vs. 5.5%, p=0.001).
A total of 79 (24.2%) patients with limitations on life support survived to hospital discharge. Table 2e (ESM) reports the characteristics of patients with limitations to life support according to survival. Patients who survived had fewer limitations on life support; all limitations on life support in this group involved withholding life-support measures, not withdrawing them. The most common reason for decisions to limit life support was comorbidities in survivors and futility in non-survivors.
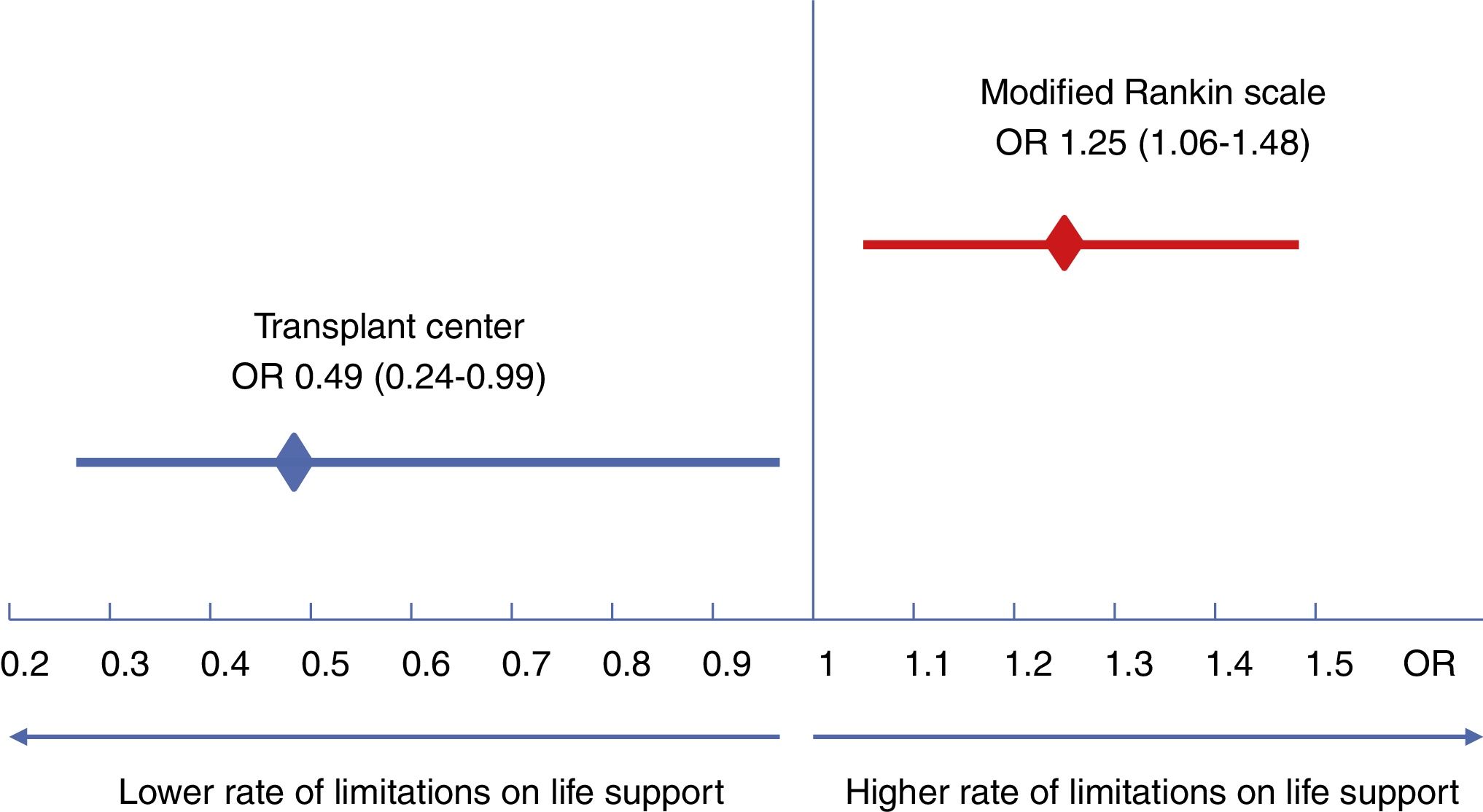
The median time from admission to the first decision to limit life support was 2 (0–7) days. Variables associated with early limitations on life support were the presence of a neurosurgical department, presence of a transplant program, age, Rankin scale, and acute condition (Table 3). However, only Rankin scale (OR: 2.5; 95% CI: 1.5–4.4) and the presence of a transplant program (OR: 0.49; 95% CI: 0.18–0.93) were independently associated with early limitations on life support (Fig. 1).
Characteristics of patients with early vs. late limitations on life support.
| LSTL ≤48hn=158 | LSTL >48hn=168 | p value | |
|---|---|---|---|
| Center characteristics | |||
| Teaching, n (%) | 112 (70.9) | 112 (66.7) | 0.61 |
| 30% staff with+10 years of experience, n (%) | 79 (50) | 75 (44.6) | 0.93 |
| 60% staff with+10 years of experience, n (%) | 77 (48.7) | 65 (38.7) | 0.15 |
| University Hospital | 90 (57) | 100 (59.5) | 0.12 |
| Hospital with Neurosurgery, n (%) | 82 (51.9) | 102 (60.7) | 0.03 |
| Hospital with transplantation programs, n (%) | 19 (12) | 37 (22) | 0.004 |
| Hospital with LSTL Protocol, n (%) | 50 (31.6) | 65 (38.7) | 0.09 |
| Patient characteristics | |||
| Age, median (p25–p75) | 77 (66–81) | 73 (63–79) | 0.014 |
| Rankin scale, median, (p25–p75) | 2 (1–3) | 1 (0–2) | 0.001 |
| Sex (male), n (%) | 100 (63.3) | 107 (63.7) | 0.84 |
| Non survival, n (%) | 138 (74.6) | 109 (77.3) | 0.57 |
| Smoking, n (%) | 26 (14.1) | 28 (19.9) | 0.16 |
| High-risk alcoholism, n (%) | 22 (11.9) | 14 (9.9) | 0.58 |
| Comorbidities | |||
| Hypertension, n (%) | 116 (36.8) | 80 (56.7) | 0.28 |
| Chronic obstructive pulmonary disease, n (%) | 68 (36.8) | 45 (31.9) | 0.36 |
| Diabetes mellitus, n (%) | 59 (31.9) | 40 (28.4) | 0.49 |
| Chronic kidney disease, n (%) | 35 (18.9) | 14 (9.9) | 0.024 |
| Liver disease, n (%) | 26 (14.1) | 14 (9.9) | 0.26 |
| Reason for admission | |||
| Cardiovascular disease, n (%) | 22 (13.9) | 25 (14.9) | 0.67 |
| Lung disease, n (%) | 29 (15.8) | 18 (10.7) | 0.17 |
| Infectious disease, n (%) | 27 (17.1) | 36 (21.4) | 0.43 |
| Digestive disorder, n (%) | 23 (14.6) | 18 (10.7) | 0.81 |
| Neurological disorder, n (%) | 25 (15.8) | 45 (26.8) | 0.12 |
| Type of limitation on life support | |||
| Conditioned intensive therapy, n (%) | 5 (3.2) | 1 (0.6) | 0.19 |
| Do not resuscitate, n (%) | 6 (3.8) | 9 (5.4) | 0.80 |
| Withhold of measures, n (%) | 116 (73.4) | 115 (68.5) | 0.34 |
| Withdraw of measures, n (%) | 31 (19.6) | 43 (25.6) | 0.11 |
The CHAID algorithm yielded a 10-node decision tree (Fig. 2). The variable most associated with early limitation on life support was the Rankin scale, and two cutoffs (≤2 and >2 points) were generated as the first line of branching. Patients with Rankin >2 have a twofold risk of early limitation on life support compared to those with Rankin ≤2.
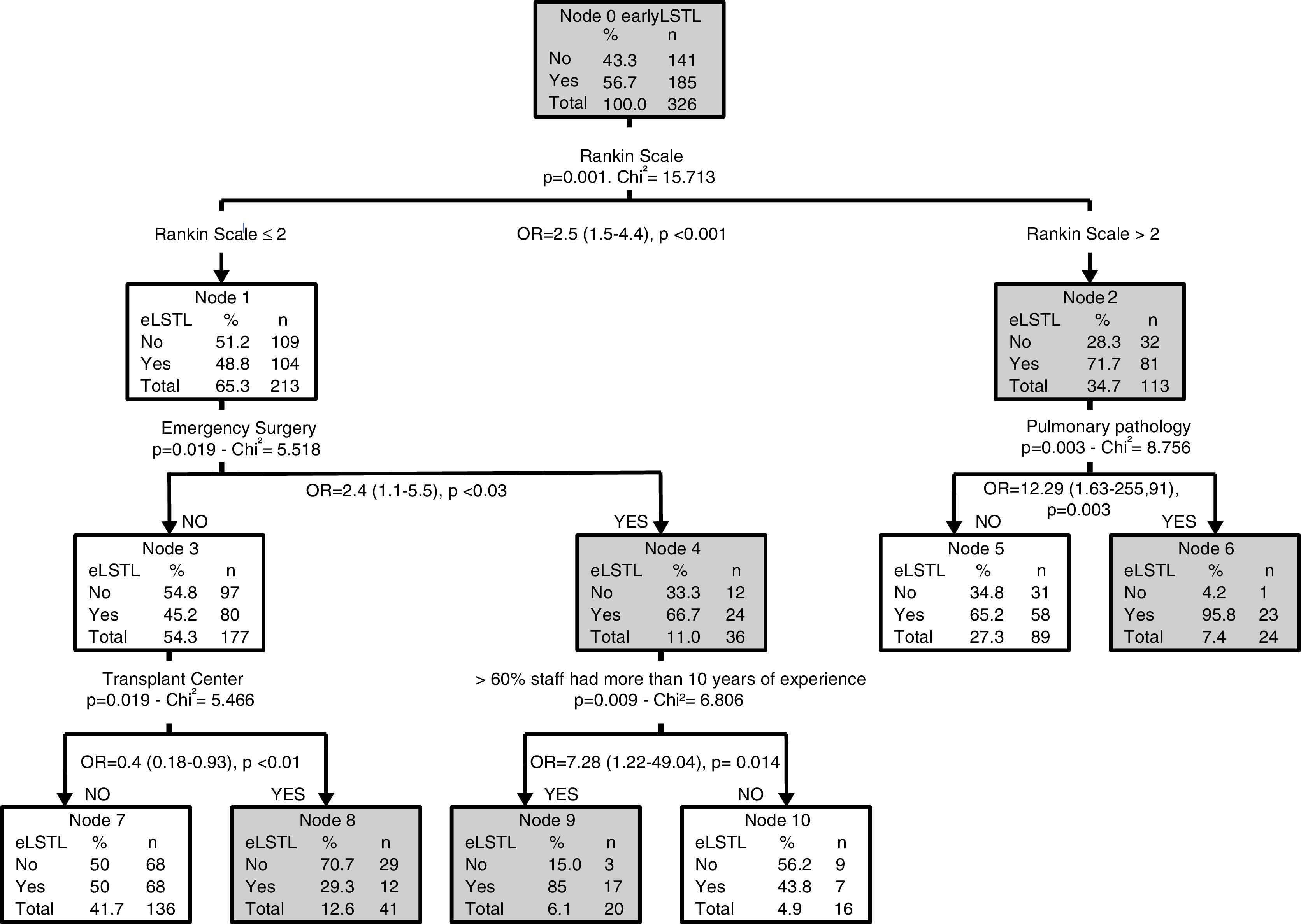
Among patients with Rankin scale >2 (n=113), 71.7% had early limitations on life support. In this group, patients with pulmonary disease had the highest rates of early limitations (OR: 12.3, 95% CI: 1.63–255.9) manifested by the strongest association in the second-line branching. Of these patients, 87% had been admitted for an acute recurrence of their chronic process, and the first limitation on life support consisted of withholding measures in 82.6%. In this group of patients, survival was 34.8%.
Among patients with Rankin ≤2 (n=213), the rate of early limitations on life support was 48.8%. At this partition level, emergency surgery was the most important variable associated with early limitation in the second-line branching; the rate was higher in patients who had undergone emergency surgery (66.7%) vs. in patients without emergency surgery (45.2%, p=0.019). In 75% of emergency surgery patients, the procedure was done for a complicated abdominal process (4 suture dehiscence, 9 peritonitis, and 5 intestinal ischemia). The median age of these patients was 77 (66–81) years, and 33.3% had active cancer. Among patients with Rankin <2 and emergency surgery, staff experience was the most important variable in the third-line branching. Centers where more than 60% of the physicians had more than 10 years of experience were associated with a higher probability of early limitations on life support. By contrast, in the subgroup of patients that did not undergo emergency surgery, the rate of early limitations was 45.2%. In the third branch, if the patient was admitted to a transplant center, the rate of early limitations was lower (29%).
DiscussionThe CHAID model elucidated multilevel interactions among risk factors that enable us to elaborate a decision tree to identify risk factors for early limitations on life support. In the first level of partition, quality of life had the strongest association with early limitations on life support.
Limitations on life support were applied most frequently in patients with medical (rather than surgical or traumatic) conditions, acute (rather than chronic) disease, and neurological diagnoses. We found that the first limitation consisted of withholding measures in 70.9% of patients, corroborating reports from previous studies.16–18 One in four patients with limitations on life support survived to hospital discharge, similar to the survival rate published recently by Lobo et al.,19 although lower than the rates reported in other studies.18,20 These differences could be explained by the differences in the definitions of limitations on life support and in the characteristics of the patients included in the studies.
Limiting life support is a common practice in Spanish ICUs.21 In our study, 71.8% of the patients who died had limitations on life support; this is much larger than the 41.3% in a multicenter study in Spain reported recently by Estella et al.22 However, only one-fifth of the patients who died in that study received cardiopulmonary resuscitation, suggesting that some kind of limitation was applied in most patients. Our findings regarding the limitation of life support are similar to those reported in most European countries; however, limitations are applied much more frequently in Scandinavia.20
Numerous studies have shown that end-of-life decisions are affected by various factors, including geographical,8,23 religious, cultural,8,24 and legal25 factors, patient-related factors,26 institutional characteristics,23,26,27 and even differences among the professionals involved in decision making.28 In a systematic review, Mark et al.29 found substantial variability between world regions, between countries, within countries, and even between intensivists within a single ICU; our results show that the differences in a small geographical area are similar to those seen across the world. We found wide variability among centers in the approach to limitations, with the percentage of patients in whom life-support measures were withheld ranging from 12.9% to 72.73% and the percentage of patients in whom life-support measures were withdrawn ranging from 0% to 47.37%.
Few studies have looked in depth at patient-related and staff-related factors that determine the timing of limitations on life support. Unlike some studies,8,21 we found that age was not a determining factor in end-of-life decisions within 48h of ICU admission. Our CHAID analysis showed that patients with worse modified Rankin scale scores on ICU admission are more likely to have early limitations on life support. Within this subgroup, patients with lung disease accounted for a higher proportion of early limitations, and limitations largely consisted of withholding measures, most often orotracheal intubation. Noninvasive mechanical ventilation improves survival in COPD exacerbation,30 and it is becoming more common in patients in whom orotracheal intubation is not indicated.31–33 Azoulay et al.33 found lower mortality in patients with COPD in whom orotracheal intubation was withheld (34% vs. 51% in patients without COPD in whom orotracheal intubation was withheld, p=0.01). Noninvasive ventilation could explain why more than one-third of patients admitted for acute recurrence of chronic lung disease who had early limitations on life support survived to hospital discharge.
In the subgroup of patients with better modified Rankin scores on ICU admission, patients admitted after emergency surgery had a higher proportion of limitations on life support, and these findings differ from those of other studies. Few studies have analyzed end-of-life care in surgical patients. One multicenter study analyzing the timing of limitations on life support found that surgical patients had a lower rate of limitations within one week of admission than medical patients.34 The preference for maintaining life-support measures in patients admitted for surgical reasons has been attributed to a “covenant of care” between surgeons and their patients.35 A survey revealed that most surgeons in the United States refused to operate on patients who did not agree to receive life-support measures during the postoperative period, and only half of surgeons agreed to withdraw life support before day 14 of admission.36 In our study, emergency surgery (not scheduled, as in previous studies) was associated with early limitations on life support. The median age of patients receiving early limitations was 77 years, and up to one-third had active cancer.
In patients admitted after emergency surgery, early limitations were also more common in ICUs with a greater proportion of highly experienced physicians. We can only speculate on the reason for these findings. Perhaps greater experience makes physicians more effective at communicating with patients and their families, and this could have an impact on early decision making.37
In patients who were not admitted after emergency surgery, early limitations on life support were less common at centers that perform transplants than in those that do not (29.3% vs. 50%, p=0.001). This could be explained because more than half the patients admitted to ICUs in transplant centers had neurological disease (data not shown). As our group published elsewhere, early limitations in this group of patients are controversial and these patients should be carefully observed for a few days before making end-of-life decisions.38
Clinical practice guidelines recommend multidisciplinary participation in end-of-life decisions.3,5,39 In our study, the consensus among physicians was 97.2%; however, nursing team participation was remarkably lower (57.1%), although much higher than the 24.5% observed in participated study carried out in 84 Italian ICUs.40 The nursing team's participation in end-of-life decisions is essential as it helps improve understanding of the patient's values and social circumstances. All professionals should attend sessions where end-of-life decisions are taken; full participation may require changes to the organization of healthcare to enable greater participation by nurses. Moreover, healthcare teams should reach decisions together with patients and/or family through a process of deliberation, choosing between different options, conforming better to patients’ interests.41 In our study, consensus with the family was reached in 84% of cases.
The present study has several limitations. All participating hospitals were located in the same region, so caution in warranted in extrapolating our findings to other areas. Nevertheless, the large number of cases allows us to extract important data about end-of-life decisions in our environment and about the influence of different variables on decision making. Moreover, team physicians were not blinded to the study; simple observation can involve attitude changes, so we cannot rule out that the study itself may have influenced some decision. However, all the participating centers have extensive experience in end-of-life decisions, and the impact of observation on decision making was probably minimal. Furthermore, although we recorded information about consensus patients’ advance life directives and families’ agreement, we did not specifically record patients’ opinions. However, only 59 patients (18.1%) were conscious when the decision to limit life support was taken. Another limitation is that, at the time of the study, only 3 centers had protocols for limiting life support. The absence of protocols could very well affect our results; however, our main objective was to study how decisions to limit life support were made. Our results show the need for educational interventions to encourage all centers to develop protocols for limiting life support.
Another potential limitation is that we were unable to analyze the impact of severity scores because different scores were used at different centers. Severity scores can identify groups of patients with a high risk of death,7,9 but cannot identify individual risk; moreover, severity at admission is not a reason for limiting life support.33,37 Because we only recorded the characteristics of patients who died or had limitations on life support, we cannot determine whether there were important differences between these patients and the rest of the patients admitted to the ICUs; however, this comparison, although interesting, was not an objective of this study. Finally, although the CHAID algorithm we developed is potentially very useful, the large number of terminal nodes may result in information overload and make it difficult to use. Nevertheless, we imposed a very strict model and required each node to include at least 20 patients so that the resulting tree could be easily interpreted.
In conclusion, this prospective multicenter study corroborated that limitations on life support are common in ICUs. The main factor guiding the decision to limit life support within 48h of admission was quality of life at ICU admission. Our CHAID tree analysis found that age and comorbidities (except COPD) seem to play no role in early decisions to limit life support and that patient-related, center-related, and teamwork-related factors also affect end-of-life decisions.
Author contributionsVB, AS, MB conceived and designed the study. All authors contributed to the acquisition and local preparation of the constituent database.
AR and VB performed the analysis of the data and the CHAID model.
All authors made important intellectual contributions and actively participated in the interpretation of the data and wrote the paper. All authors contributed to critical examination of the paper for important intellectual content and approval of the final manuscript.
Conflicts of interestThe authors declare that they have no conflicting interests.
The authors would like to thank John Giba for rewriting the manuscript to improve clarity and readability.
The following are the supplementary data to this article:


