


Airway management is of utmost importance to every anesthesiologist. The technique of choice is orotracheal intubation with direct laryngoscopy.1 Determinants of orotracheal intubation include airway anatomical configuration and the type of devices and techniques used.2 In 1897 Kirstein performed the first comparison between two positions for airway management. This comparison was followed by Chevalier Jackson's description of the neck extension and full hyperextension positions performed by his assistant during surgery in 1913. Magill (1932) described that a patient during tracheal intubation adopts a position as if he/she were to sniff and Bannister and McBeth (1944) described the three-axes theory which postulates that an alignment of the oral, pharyngeal and laryngeal axes was necessary to achieve an adequate glotic opening.3 However, a recent magnetic resonance imaging study on airway configuration suggests that such theory cannot be proven and proposes another method to assess objective measures for airway evaluation.4
Some studies have suggested that the use of an interscapular support with hyperextension improves airway configuration for laryngoscopy.1,5 However, this position has never been compared to the generally accepted sniffing position described by Magill.6
The aim of this study was to compare airway configurations of healthy volunteers measured as α angle and area under the line of site between the use of an interscapular support with hyperextension and sniffing positions. We wished to measure the differences of these two values between both positions.
After institutional and local ethics committee approval we performed six magnetic resonance imaging (MRI) studies on three healthy (no difficult airway risk factors) volunteers. Each volunteer was evaluated with both interscapular support with hyperextension and sniffing positions. T1-weighted images in the sagittal plane were obtained with a 1.5T Magnetom Vision MRI scanner (Siemens Medical Solutions, Erlangen, Germany). The interscapular support with hyperextension position was achieved by placing a 10cm height and 8cm width non-collapsible rubber device covered with silicone. The sniffing position was achieved by elevating the occiput 10cm and extending the head at the atlanto-occipital joint. The images were analyzed with OsiriX 5.0.2 DICOM viewer for MacOS.
Two Bézier splines were measured as described by Greenland.4 We used the slide that corresponded to the medial line as confirmed by both a radiologist and an otorhinolaryngologist. The splines were drawn starting at the tip of the top front incisors, through the middle of the airway passage, at the junction of the hard and soft palates, at the lever of the tip of the epiglottis, at the glottis, and the trachea at the level of the seventh vertical vertebra (Fig. 1). This created 2 curves, one that represents the oro-pharyngeal airway (curving toward the right) and one that represents the pharyngo-glotto-tracheal airway (curving toward the left). A line was drawn at the point where the two curves met and the angle formed by this line and the horizontal one was calculated (α angle). In addition, we measured the area between the first curve and a straight line that was drawn from the tip of the top front incisors to the middle of the glottis (representing the line of sight). The data from the two position groups were compared descriptively.
. The intersection between a horizontal line and a line drawn at the point where the two curves intersect, define the angle α (A=33.03°, B=5.97°).")
Magnetic resonance imaging scans of a single volunteer. Panel A shows the interscapular support with hyperextension position and Panel B shows the sniffing position. The closed polygons depict the area between the oro-pharyngeal airway and the line of site (A=43.60cm2, B=37.90cm2). The intersection between a horizontal line and a line drawn at the point where the two curves intersect, define the angle α (A=33.03°, B=5.97°).
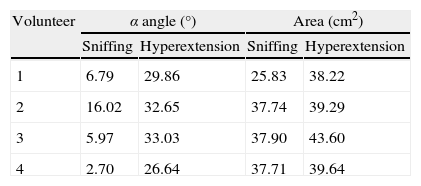
The results of the measurements of α angle and area under the line of sight are shown in Table 1. These suggest that smaller angles and areas are obtained with the sniffing position as compared to the interscapular support with hyperextension position.
To our knowledge, the comparison between the sniffing and interscapular support with hyperextension positions had not been previously reported in the literature. In recent years, different studies have compared the sniffing position with other positions of the head and neck with apparently conflicting results.3,7,8 The sniffing position has not been found to be superior to the simple extension of the neck during direct laryngoscopy in patients requiring elective surgery.9 However, differences have been found when approaching obese patients and those with limited neck movement. In one study of obese patients requiring bariatric surgery the ramped position had a better performance than the sniffing position.9–11
In conclusion, the use of an interscapular support with hyperextension position increases objective measures related to airway configuration. While these increases are not desirable for subjects without risk factors for difficult airway, it could provide an alternative approach for the management of the airway of obese patients.
Funding disclosureThis study was carried out with funds of the Departments of Anesthesiology and Magnetic Resonance Imaging, Hospital de San Jose, Bogota.
Conflicts of interestThe authors declare no conflicts of interest.
We would like to honor the work of Astrid A Amezquita, MD, Faculty of Medicine, Fundacion Universitaria de Ciencias de la Salud, Bogota, Colombia, who was part of the research team and who died during the course of this study. She participated in the design and analysis of this study, therefore she is considered as a coauthor.

