

Analizar los factores asociados al shock vasopléjico en el postoperatorio de cirugía cardiaca. Analizar la influencia de la vasopresina como terapia de rescate al tratamiento de primera línea con noradrenalina.
DiseñoEstudio de cohortes, prospectivo y observacional.
ÁmbitoUCI de postoperatorio cardiaco de un hospital de tercer nivel.
PacientesPacientes sometidos a cirugía cardiaca con ingreso posterior en la UCI desde enero de 2021 hasta diciembre de 2022.
IntervencionesRegistro de variables clínicas prequirúrgicas, perioperatorias y al alta de UCI.
Variables de interés principalesTratamiento crónico, presencia de shock vasopléjico, necesidad de vasopresina, tiempo de circulación extracorpórea, mortalidad.
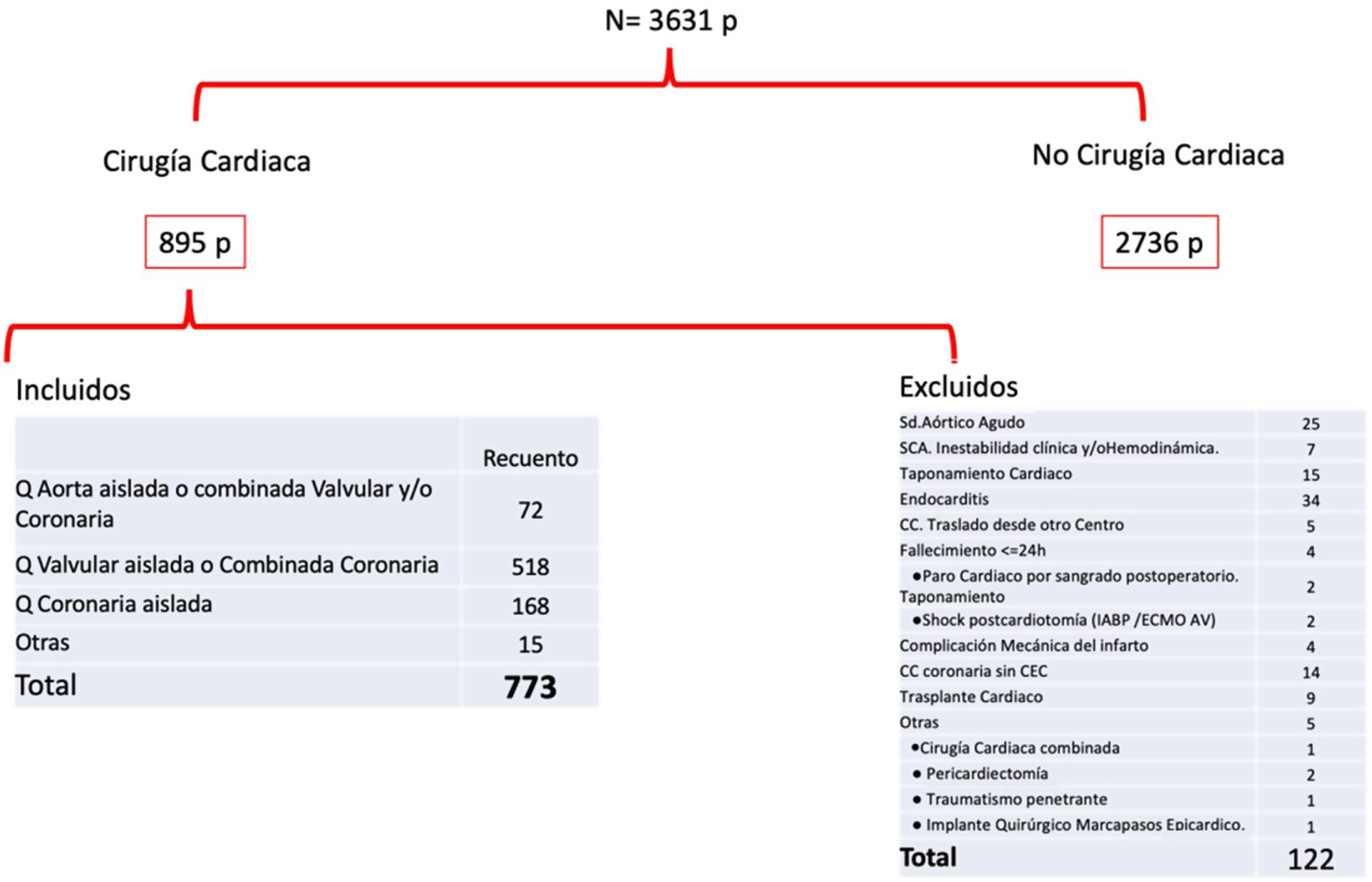
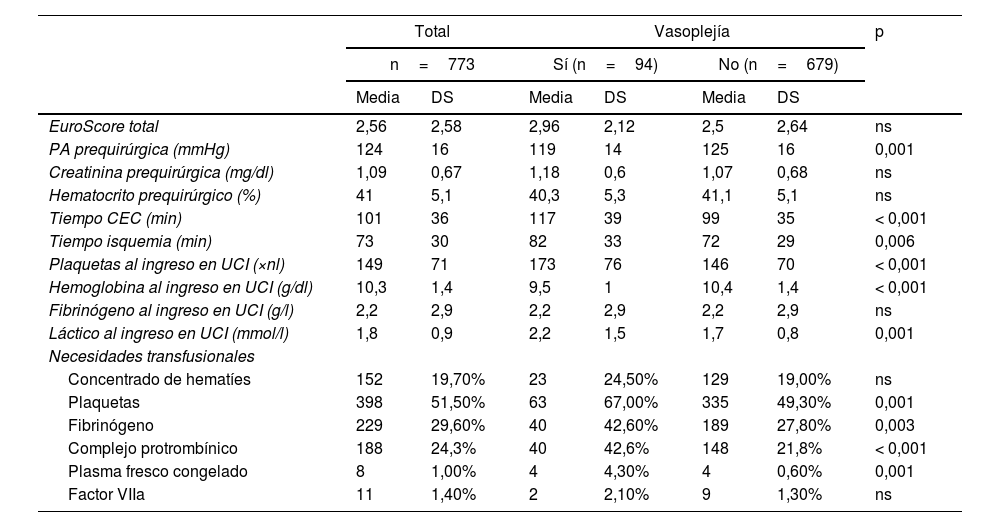
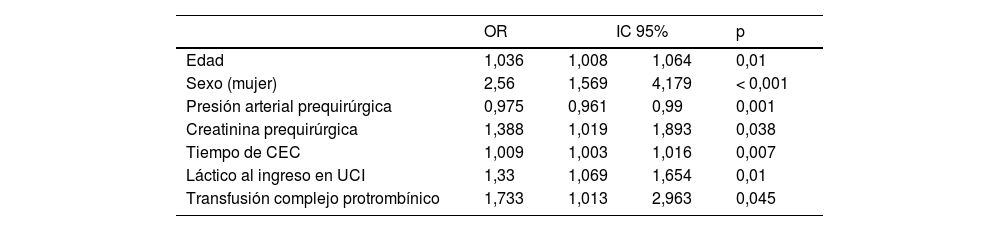
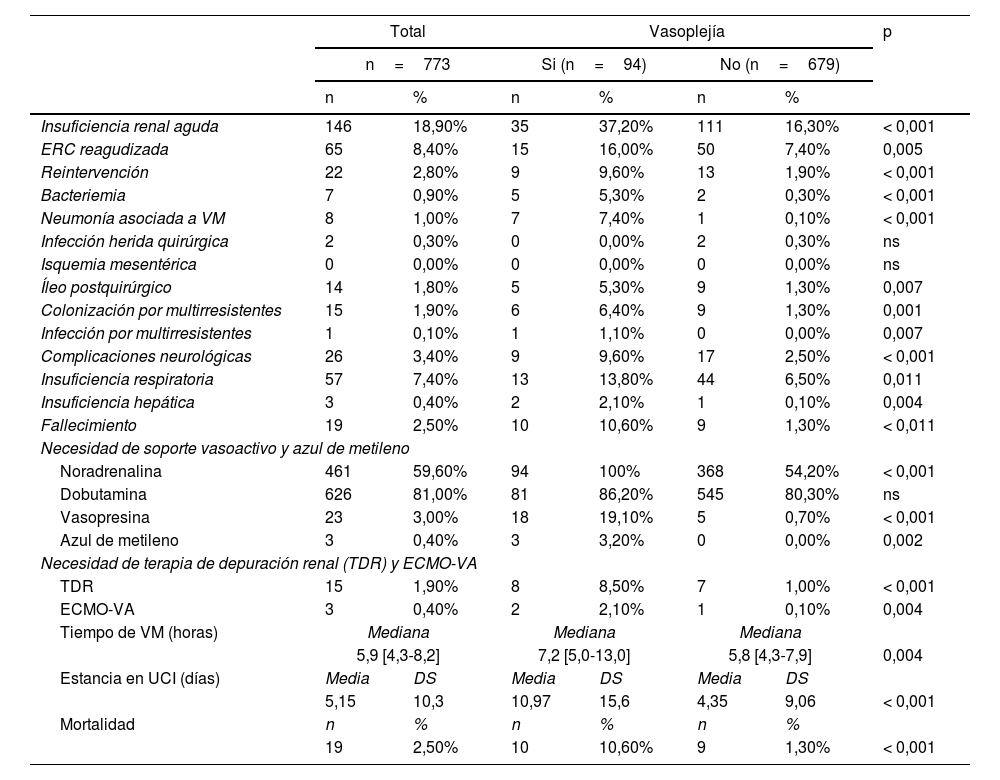
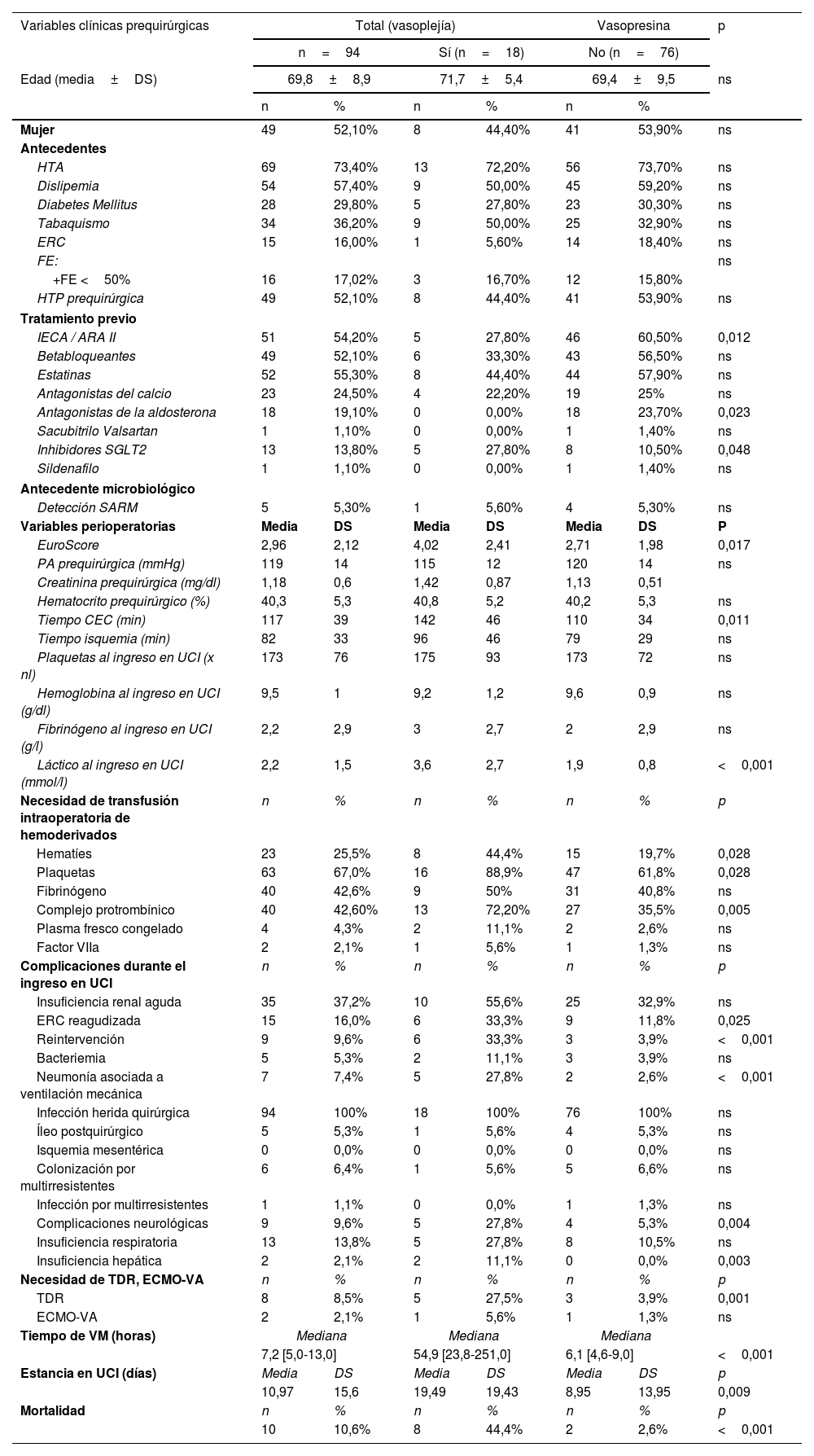
Resultados773 pacientes cumplieron los criterios de inclusión. La edad media fue 67,3años, predominio del sexo masculino (65,7%). Se documentó vasoplejía post-CEC en 94 pacientes (12,2%). La vasoplejía se asoció independientemente con edad, sexo femenino, creatinina prequirúrgica, tiempo de circulación extracorpórea, lactato al ingreso en la UCI y necesidad de complejo protrombínico. De los pacientes que desarrollaron vasoplejía, 18 (19%) precisaron vasopresina de rescate, asociándose con la toma prequirúrgica de IECA/ARAII, peor EuroScore y mayor tiempo de circulación extracorpórea. La vasoplejía refractaria con necesidad de vasopresina se asoció a aumento de la morbimortalidad.
ConclusionesLa vasoplejía post-circulación extracorpórea se asocia a aumento de morbimortalidad. Acortar tiempos de circulación extracorpórea y minimizar las necesidades transfusionales podría disminuir su desarrollo. Retirar IECA y ARAII previa a la cirugía podría reducir la incidencia de vasoplejía refractaria con necesidad de rescate con vasopresina. El tratamiento de primera línea de este síndrome es la noradrenalina, si bien el rescate con vasopresina es un buen complemento en situaciones de refractariedad.
Analizing associated factors with vasoplegic shock in the postoperative period of cardiac surgery. Analizing the influence of vasopressin as rescue therapy to first-line treatment with norepinephrine.
DesignCohort, prospective and observational study.
SettingMain hospital postoperative cardiac ICU.
PatientsPatients undergoing cardiac surgery with subsequent ICU admission from January 2021 to December 2022.
InterventionsRecord of presurgical, perioperative and ICU discharge clinical variables.
Main variables of interestChronic treatment, presence of vasoplegic shock, need for vasopressin, cardiopulmonary bypass time, mortality.
Results773 patients met the inclusion criteria. The average age was 67.3, with predominance of males (65.7%). Post-CPB vasoplegia was documented in 94 patients (12.2%). In multivariate analysis, vasoplegia was associated with age, female sex, presurgical creatinine levels, cardiopulmonary bypass time, lactate level upon admission to the ICU, and need for prothrombin complex transfusion. Of the patients who developed vasoplegia, 18 (19%) required rescue vasopressin, associated with pre-surgical intake of ACEIs/ARBs, worse EuroScore score and longer cardiopulmonary bypass time. Refractory vasoplegia with vasopressin requirement was associated with increased morbidity and mortality.
ConclusionsPostcardiopulmonary bypass vasoplegia is associated with increased mortality and morbidity. Shortening cardiopulmonary bypass times and minimizing products blood transfusion could reduce its development. Removing ACEIs and ARBs prior to surgery could reduce the incidence of refractory vasoplegia requiring rescue with vasopressin. The first-line treatment is norepinephrine and rescue treatment with vasopressin is a good choice in refractory situations. The first-line treatment of this syndrome is norepinephrine, although rescue with vasopressin is a good complement in refractory situations.
Article
Go to the members area of the website of the SEMICYUC (www.semicyuc.org )and click the link to the magazine.


