

Disease produced by SARS-CoV-2 has often been compared with that caused by influenza virus. In fact, considering its spreading capacity and the relatively low lethality rates initially reported in China, SARS-CoV-2 was thought to be more similar to the flu than SARS-CoV-1. However, it is important to understand that disease produced by SARS-CoV-2 is not the flu.1,2
Few studies have directly compared the characteristics of patients requiring admission to the Intensive Care Unit (ICU) in the SARS-CoV-2 pandemic and flu epidemics. In this regard, important differences are likely to be found between the two respiratory viral infections, including the required supportive measures, the proportion of individuals that develop severe illness, and the in-ICU mortality rates.3–5
Evaluation of the characteristics, prescribed treatments, outcomes and mortality rates of the two diseases could be used to improve future prognostic assessments and planning in ICUs.6
The present study compares the population admitted due to COVID-19 and flu in the decade 2009–2019, based on the data from an ICU in a tertiary university hospital, and evaluates the differences in terms of risk factors, clinical characteristics, treatments and outcomes.
A retrospective, analytical comparative study was made between patients admitted to the ICU with influenza virus infection in the period September 2009–April 2019 and patients admitted due to SARS-CoV-2 infection between March and December 2020. The analysis was based on the respective registries, with prior approval from the local Ethics Committee and the obtainment of informed consent from the patient or representative where so required by the Committee. The data are reported as numbers and percentages, or as the mean and standard deviation (SD). Qualitative and quantitative variables were compared using the χ2 test and the Student t-test, respectively. Statistical significance was considered for p ≤ 0.05.
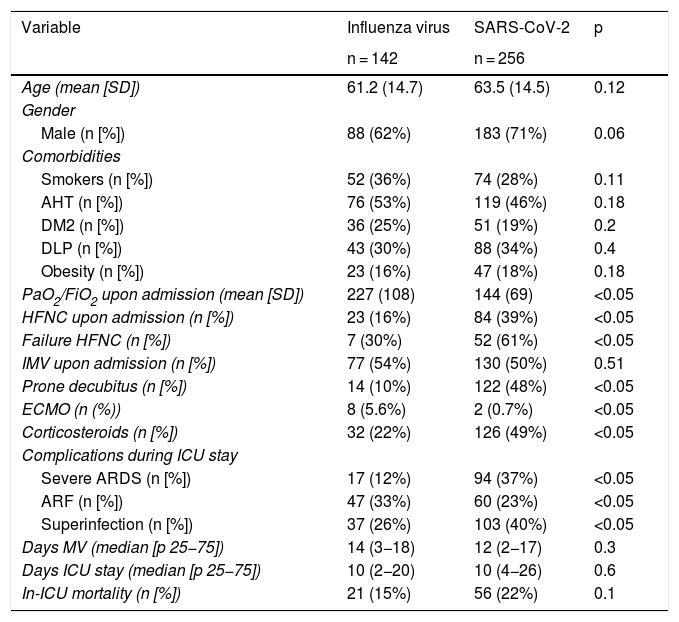
During the mentioned study period, a total of 142 and 256 patients with influenza virus infection and SARS-CoV-2 infection were admitted, respectively. There were no significant differences between the two groups in terms of age and gender or comorbidities (Table 1). The PaO2/FiO2 ratio upon admission was significantly lower among the SARS-CoV-2 cases (144 vs. 227; p < 0.05), with no differences being observed in the need for invasive mechanical ventilation (IMV) upon admission (first 24 h of ICU stay). A significantly lower tidal volume (TV) was used in the SARS-CoV-2 group (465 vs. 495; p < 0.05), with a higher positive end-expiratory pressure (PEEP) (11 vs. 7; p < 0.05).
Principal characteristics of the cohort of patients admitted to an Intensive Care Unit due to influenza virus infection and the patients admitted due to SARS-CoV-2 infection.
| Variable | Influenza virus | SARS-CoV-2 | p |
|---|---|---|---|
| n = 142 | n = 256 | ||
| Age (mean [SD]) | 61.2 (14.7) | 63.5 (14.5) | 0.12 |
| Gender | |||
| Male (n [%]) | 88 (62%) | 183 (71%) | 0.06 |
| Comorbidities | |||
| Smokers (n [%]) | 52 (36%) | 74 (28%) | 0.11 |
| AHT (n [%]) | 76 (53%) | 119 (46%) | 0.18 |
| DM2 (n [%]) | 36 (25%) | 51 (19%) | 0.2 |
| DLP (n [%]) | 43 (30%) | 88 (34%) | 0.4 |
| Obesity (n [%]) | 23 (16%) | 47 (18%) | 0.18 |
| PaO2/FiO2 upon admission (mean [SD]) | 227 (108) | 144 (69) | <0.05 |
| HFNC upon admission (n [%]) | 23 (16%) | 84 (39%) | <0.05 |
| Failure HFNC (n [%]) | 7 (30%) | 52 (61%) | <0.05 |
| IMV upon admission (n [%]) | 77 (54%) | 130 (50%) | 0.51 |
| Prone decubitus (n [%]) | 14 (10%) | 122 (48%) | <0.05 |
| ECMO (n (%)) | 8 (5.6%) | 2 (0.7%) | <0.05 |
| Corticosteroids (n [%]) | 32 (22%) | 126 (49%) | <0.05 |
| Complications during ICU stay | |||
| Severe ARDS (n [%]) | 17 (12%) | 94 (37%) | <0.05 |
| ARF (n [%]) | 47 (33%) | 60 (23%) | <0.05 |
| Superinfection (n [%]) | 37 (26%) | 103 (40%) | <0.05 |
| Days MV (median [p 25−75]) | 14 (3−18) | 12 (2−17) | 0.3 |
| Days ICU stay (median [p 25−75]) | 10 (2−20) | 10 (4−26) | 0.6 |
| In-ICU mortality (n [%]) | 21 (15%) | 56 (22%) | 0.1 |
AHT: arterial hypertension; SD: standard deviation; DM2: type 2 diabetes mellitus; DLP: dyslipidemia; HFNC: high-flow nasal cannula; IMV: invasive mechanical ventilation; ECMO: extracorporeal membrane oxygenation; ARDS: acute respiratory distress syndrome; ARF: acute renal failure. p 25–75: percentile 25–75.
Our analysis reflects a similar patient profile regarding age, gender and comorbidities in both infections. However, their respiratory impact differed in terms of the percentage of patients requiring mechanical ventilation, with different oxygenation levels upon admission, and differences in the required ventilatory parameters.
In this regard, although admission to the ICU could take place in different evolutive moments of each of the infections, a number of authors suggest that there may be differences in the type of acute respiratory distress syndrome (ARDS) seen in COVID-19.7 In fact, necropsy studies indicate that alveolar microthrombosis and vascular angiogenesis are more frequent among COVID-19 cases than in patients with the flu.8 However, the histological characteristics seen in COVID-19 appear to be indistinguishable from those observed in other causes of diffuse alveolar damage.9
Although previous studies have recorded greater mortality in seriously ill patients who develop ARDS in the context of influenza virus infection than in those with ARDS secondary to COVID-19,10 there have been recent reports of poorer respiratory outcomes and a greater in-hospital mortality risk in patients with COVID-19, independently of age, gender and the ICU severity scores.5
Our study has a number of limitations. It involves a relatively small sample from a single hospital, and there are weaknesses derived from the long time period of the flu series. On the other hand, the results corresponding to the COVID-19 group were obtained at the height of the pandemic, with saturation of the healthcare services, and sometimes involving medical and nursing staff with little experience in this scenario.
Based on our data, it can be concluded that the analyzed therapies and characteristics in the patients with flu and those with COVID-19 differ upon admission to the ICU, and that differences in outcome are moreover also observed.
Financial supportNone.
Conflicts of interestThe authors declare that they have no conflicts of interest in relation to the present study.
Please cite this article as: González-Castro A, Fernandez-Rodríguez A, Cuenca Fito E, Suberviola-Cañas B, Peñasco Y, Rodríguez-Borregán JC. Comparación de las características de los pacientes con enfermedad por coronavirus tipo 2 y la gripe estacional ingresados en una unidad de cuidados intensivos. Med Intensiva. 2022;46:226–228.

