

Recent publications1,2 show that it is necessary to increase the monitoring of patients admitted to conventional hospital wards in an attempt to avoid any clinical impairments, whether by administering the right therapy or by improving the monitoring methods by taking them to an intensive care unit (ICU). It has been established that different systems or algorithms for severity identification purposes reduce adverse events, prevent the appearance of cardiorespiratory arrests (CRA), and improve prognosis.
The main methods used to achieve this goal have been the creation of rapid response teams (with different specialists and activation systems)3–6 and models of ICUs without walls7–10 (combined effort from different professionals and automated detection of severity by integrating clinical and lab variables). However, some publications show contradictory results possibly due to the heterogeneity of the activation.
This need for a better monitoring control is essential if we want to manage certain groups of patients, such as patients discharged from ICUs, patients in the immediate postoperative period, or patients with sepsis; but, also medical patients in life-threatening situations while they remain hospitalized in conventional wards.
We know that conventional hospital wards are filled with patients with potentially serious conditions and that for every hour delayed during a patient's admission to an ICU, there is a 1.05 per cent chance of dying at the hospital,11 as a matter of fact, patients requiring ICU admissions have worse prognoses the longer they wait on their hospital admission.12 It was a long time ago when it was established that patients suffering from hospital CRAs showed altered vital signs that could have been detected up to 72h prior to the event, making CRAs potentially reversible.
It is very interesting to see how, recently, van Galen13 showed that although physiological alterations and alarms are detected in the patients’ vital signs, these are not always taken care of adequately or escalated to a higher healthcare provider. Oddly enough, the main reason for all activation delays has nothing to do with a failing healthcare structure, but with issues with the team's performance and identification of these alterations. This means that it is essential for the emergency medical services to create not only clear identification patterns for patients with higher risks of clinical impairment or who suffered from a CRA, but also clinical activation algorithms.
Recently, in the case of septic patients, great effort has been made to change the definition, and basically to establish one user-friendly tool in clinical practice in order to identify patients with higher hospital death rates using the qSOFA score. This indicator allows us to identify what patients with clinical suspicion of infection have mortality rates >10 per cent with an AUROC ranking 0.80 for patients admitted outside the ICU. This is how we know that patients scoring >2 in the qSOFA score amount to 70 per cent of the patients who die due to sepsis.14,15
The qSOFA score, which is nothing but a quick system to detect multi-organic dysfunctions, is not only useful in patients with clinical suspicion of infection, but also when applied to all patients admitted to conventional wards, since it is capable of detecting patients with higher chances of having worse prognoses with an AUROC ranking 0.70.16
Probably, the use of a system so simple as the qSOFA score would be useful for the monitoring and identification of patients with risk of clinical impairment in conventional wards. Recently Churpek et al. compared different risk identification systems to the qSOFA score in conventional wards. They established that systems such as the Early Warning Score (EWS) and, particularly, the HEWS score both improve the qSOFA score predicting abilities for all hospitalized patients.17
Therefore, it seems clear to us that in order to improve the management of patients admitted to conventional wards we should establish risk groups of poor prognosis. We can establish these groups using the EWS systems (that we think should be adapted to the common monitoring protocols used) (Tables 1 and 2). These systems allow the creation of task escalation algorithms by the nursing team, the doctors on call, or the rapid response teams, which in turn allows us to improve the monitoring capabilities or management of these higher risk patients.
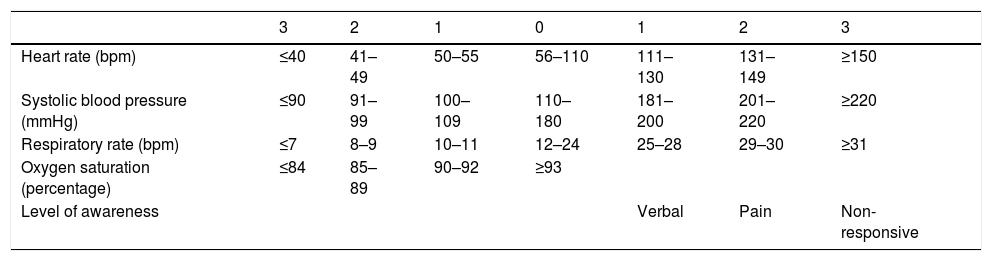
Local adaptation of the EWS system in the Hospital Universitario del Henares (Henares Early Warning Score [HEWS]) created by the Intensive and Internal Medicine Unit.
| 3 | 2 | 1 | 0 | 1 | 2 | 3 | |
|---|---|---|---|---|---|---|---|
| Heart rate (bpm) | ≤40 | 41–49 | 50–55 | 56–110 | 111–130 | 131–149 | ≥150 |
| Systolic blood pressure (mmHg) | ≤90 | 91–99 | 100–109 | 110–180 | 181–200 | 201–220 | ≥220 |
| Respiratory rate (bpm) | ≤7 | 8–9 | 10–11 | 12–24 | 25–28 | 29–30 | ≥31 |
| Oxygen saturation (percentage) | ≤84 | 85–89 | 90–92 | ≥93 | |||
| Level of awareness | Verbal | Pain | Non-responsive |
The HEWS score is a local adaptation created by the Intensive and Internal Medicine Unit following the Early Warning Score (EWS) algorithms for the early detection of severity, and it is vital signs-based. The score goes from lowest (0 points) to highest severity (3 points), and uses five physiological parameters: heart rate (beats per minute), systolic blood pressure (mmHg), respiratory rate (breaths per minute), oxygen saturation (percentage), and response level to different stimuli. The overall score (0–15 points) is associated with the patient's estimated severity code, and activates one hospital decision-making algorithm – the HEWS protocol.
Hospital decision-making algorithm based on the overall HEWS score.
| ≥7 urgent or isolated value≥3 | Call the ICU immediately (except for LSL) |
| ≥5–6 warning | Contact doctor on call |
| ≤4 observation | Check vital signs every 8h |
Task escalation algorithm-protocol based on the HEWS score algorithm. Scores ≤4 speak to us about low severity, being the check-up of vital signs recommended every 8h followed by observation. Scores between 5 and 6 show intermediate severity, and warn the doctor on call who then starts the decision-making process. Scores ≥7 or isolated scores of 3 immediately activate the rapid response team which is led by the intensivist and includes the participation of the patient's treating physician, except for cases previously defined as palliative care cases.
From here on, these vital sign-based algorithms can be improved using computerized analyses of laboratory data, biomarkers, or automated monitoring systems.
In our own experience, in order to be successful with these early detection practices, other than an adequate design, what we need to do is to raise awareness in the hospital setting by training the staff and facilitating instructional material for the easy clarification of our goals. It is also important to achieve a certain durability of the system and, to this end, it can be useful to keep open communication channels among the participating staff, and allow us to review and evaluate how the system works to later dynamically adapt the characteristics based on the context.
Somehow it seems logical to think that the degree of certainty in the detection will be higher through one “multimodal” system that includes different information channels (analytic alterations, physiological vital signs, staff, and rapid response teams), but, in our own experience, if we want to keep the motor running, we would recommend a gradual implementation of the different detection methods and areas, starting by areas where the implementation of these systems is more beneficial until the necessary learning curve is achieved.
Based on the aforementioned findings and the experience accumulated so far, the implementation of detection methods, alert, and early responses improve both the clinical results and the cost–benefit ratio, yet in order to achieve the adequate performance and durability of these systems, we need to have the compromise and involvement of different hospital agents in this project, meaning that this is one multidisciplinary approach in which it is essential to raise awareness and training.
FundingThere has been no funding whatsoever.
Conflicts of interestsThe authors of this paper declare no conflicts of interest whatsoever.
Please cite this article as: Gordo F, Molina R. Evolución a la detección precoz de gravedad. ¿Hacia dónde vamos? Med Intensive. 2018;42:47–49.

