

The major improvement in burn therapy is likely to focus on the early management of hemodynamic and respiratory failures in combination with an aggressive and early surgical excision and skin grafting for full-thickness burns.
Immediate burn care by first care providers is important and can vastly alter outcomes, and it can significantly limit burn progression and depth. The goal of prehospital care should be to cease the burning process as well as prevent future complications and secondary injuries for burn shock. Identifying burn patients appropriate for immediate or subacute transfer is an important step in reducing morbidity and mortality. Delays in transport to Burn Unit should be minimized.
The emergency management follows the principles of the Advanced Trauma Life Support Guidelines for assessment and stabilization of airway, breathing, circulation, disability, exposure and environment control.
All patients with suspected inhalation injury must be removed from the enclosure as soon as possible, and immediately administer high-flow oxygen. Any patient with stridor, shortness of breath, facial burns, singed nasal hairs, cough, soot in the oral cavity, and history of being in a fire in an enclosed space should be strongly considered for early intubation. Fibroscopy may also be useful if airway damage is suspected and to assess known lung damage.
Secondary evaluation following admission to the Burn Unit of a burned patient suffering a severe thermal injury includes continuation of respiratory support and management and treatment of inhalation injury, fluid resuscitation and cardiovascular stabilization, pain control and management of burn wound.
Los principales avances en el tratamiento de la quemadura se centran en el manejo precoz de la disfunción hemodinámica y respiratoria junto con la excisión quirúrgica agresiva y precoz y el injerto de piel en quemaduras de espesor total.
La atención inmediata a la quemadura puede cambiar el pronóstico, limitando significativamente su progresión y profundidad. El objetivo de la asistencia prehospitalaria es detener el proceso de combustión así como prevenir posteriores complicaciones y daños secundarios al shock por quemadura. Identificar los pacientes quemados subsidiarios de traslado inmediato es importante en términos de morbilidad y mortalidad. La demora en el traslado a una Unidad de Quemados de referencia debe ser minimizada.
El manejo emergente debe ser el mismo que para cualquier otro paciente politraumatizado, con evaluación y estabilización de la vía aérea, la respiración, la circulación, la discapacidad y el control ambiental.
Todos los pacientes con sospecha de inhalación deben ser trasladados del recinto tan pronto como sea posible y administrar inmediatamente oxígeno a alto flujo. Ante un paciente con estridor, dificultad para respirar, quemaduras faciales, vibrisas quemadas, tos, hollín en la cavidad oral e historia de inhalación de humo en un lugar cerrado debe ser considerada la indicación de intubación precoz. La fibroscopia puede ser útil si se sospecha daño de la vía aérea y para evaluar el daño pulmonar conocido.
La valoración secundaria tras el ingreso en la Unidad de un paciente que ha sufrido una lesión térmica grave incluye la continuación del soporte respiratorio y el manejo y tratamiento del daño por inhalación, la reanimación con líquidos y la estabilización cardiovascular, el control del dolor y el manejo de la herida.
Burns remain a major cause of traumatic injury world-wide affecting all ages. Burn injuries account for more than 300,000 deaths worldwide each year.1
Major risk factors for burns include male gender, extreme youth or old age, alcohol abuse, and substandard housing residence.
In the last half century a best understanding of the principles of care burn have resulted in improved survival rates, shorter hospital stays and decreases in morbidity and mortality rates due to the development of resuscitation protocols, improved respiratory support, infection control, early nutrition enteral and early excision and burn wound closure.2–4
Other factors, including immediate prehospital care, early emergency treatment with advanced life support capability and secondary transfer to a Burn Unit have contributed to improve substantially survival of severe burns patients.5
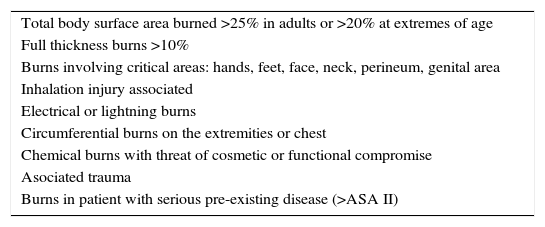
Major burns in adult patients are defined as thermal injury-induced lesions which justify intensive care treatment for at least 3 days post-injury (Table 1).6
Criteria for the diagnosis of major burns.5
| Total body surface area burned >25% in adults or >20% at extremes of age |
| Full thickness burns >10% |
| Burns involving critical areas: hands, feet, face, neck, perineum, genital area |
| Inhalation injury associated |
| Electrical or lightning burns |
| Circumferential burns on the extremities or chest |
| Chemical burns with threat of cosmetic or functional compromise |
| Asociated trauma |
| Burns in patient with serious pre-existing disease (>ASA II) |
ASA, American Society of Anesthesiologists.
The efficiency of the initial chain of medical care is essential in improving outcome, specifically in severe burns. This approach leads to a better understanding of pathophysiological mechanisms involved in burn shock.
Major burns cause massive tissue destruction and result in activation of a cytokine-mediated inflammatory response that leads to dramatic pathophysiologic effects at sites local and distant from the burn. The systemic effects occur in two distinct phases, a burn shock (ebb) phase followed by a hypermetabolic (flow) phase.
Generalized edema even in non-injured tissues occurs when the injury exceeds 25–30% total body surface area (TBSA). After major burn injury, continued loss of plasma into burned tissue can occur up to the first 48h or even longer.
Loss of intravascular fluid into burned areas and edema formation (in nonburned sites) can quickly result in burn shock with impaired tissue and organ perfusion. Thus, the initial therapeutic goal is the repletion of intravascular volume with clear fluids (isotonic crystalloids) to preserve tissue perfusion and minimize the ischemia and inflammatory responses.
This inflammatory response is the cause of an alteration in microvascular permeability in both, burned and normal tissues with resultant leakage of protein-rich fluid from intravascular to extravascular compartment.7
Edema, hypovolemia and hypoproteinaemia are the mandatory result of the fluid shifts.
The aggressive correction of this volume depletion feeds the edema, leading to a further ischemic insult.
Other factors in burn edema include the heat-induced denaturing of collagen fibers in the interstitium, causing a physical expansion of the potential third space with a transient −20 to −30mm Hg negative-pressure gradient favoring extravasation of fluid.8
Edema in the upper airway after facial, neck or upper thoracic burn and after inhalation is well known and is a clear indication of endotraqueal intubation.
The current belief is that capillary leakage that leads to fluid losses and needs for large amount of fluid therapy are mediated by anti-inflammatory mediators.
The mechanism of how these mediators act to produce this capillary integrity disruption is not known. The use of hemofiltration devices to remove such mediators has shown encouraging results.9
Other investigations have revealed that thermal injury induces massive vasoconstriction that is independent of sympathetic nervous system activity. Studies have implicated antidiuretic hormones and the renin angiotensin systems in this response.
The classic description of the burn wound and surrounding tissues is a system of several circumferential zones radiating from primarily burned tissues, with a zone of coagulation, a nonviable area of tissue at the epicenter of the burn, a zone of ischemia or stasis surrounding tissues (both deep and peripheral) to the coagulated areas, which are not devitalized initially but, due to microvascular insult, can progress irreversibly to necrosis over several days if not resuscitated properly and a zone of hyperemia, peripheral tissues that undergo vasodilatory changes due to neighboring inflammatory mediator release but are not injured thermally and remain viable. The tissues in ischemic areas, can potentially be salvaged by proper resuscitation in the initial stages.
Underresuscitation can convert this area into deep dermal or full-thickness burns in areas not initially injured to that extent.
A new area of interest with immediate resuscitation is the use of subatmospheric pressure dressings (e.g., the VAC) on affected areas. Animal models and early clinical work suggest that this treatment may limit the conversion of zones of hyperemia to zones of ischemia by removing edematous fluid and allowing salvage of areas that would otherwise need excision and grafting.8
Without effective and rapid intervention all severe burns suffer burn shock. Burn shock is a unique combination of distributive and hypovolemic shock.
Adequate resuscitation is the single most important therapeutic intervention in burn treatment. Recent evidence suggests that timely fluid resuscitation can significantly reduce multiorgan failure and mortality in thermally injured patients.
A rapid determination of percentage TBSA burn and calculation of the fluid requirements can be difficult and often incorrect when the person treating these burns is an inexperienced clinician. The error in estimating burn extent and depth result in significant under- or overcalculation of fluid requirements.2,9
Prehospital care and Emergency Department CareThe quality of prehospital care is probably of prime importance in reducing both the local and systemic effects of burn injury.
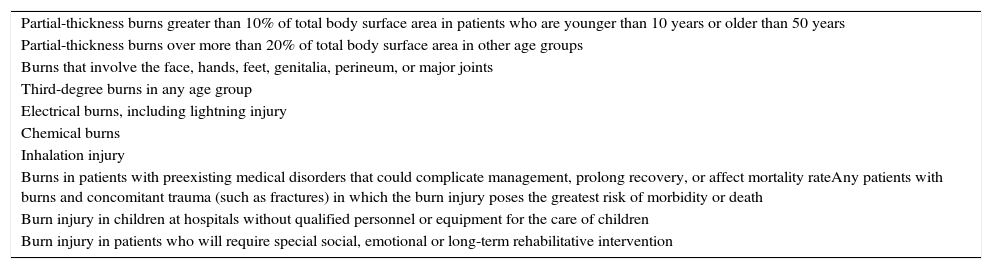
Identifying burn patients appropriate for immediate or subacute transfer is an important step in reducing morbidity and mortality. The American Burn Association (ABA) has established recommended criteria for transfer to burn centers. These criteria recognize the factors that are associated with poorer outcomes, such as advanced age, electrical burns, and smoke inhalation (Table 2).
Criteria for referral to a Burn Unit. American Burn Association (ABA).
| Partial-thickness burns greater than 10% of total body surface area in patients who are younger than 10 years or older than 50 years |
| Partial-thickness burns over more than 20% of total body surface area in other age groups |
| Burns that involve the face, hands, feet, genitalia, perineum, or major joints |
| Third-degree burns in any age group |
| Electrical burns, including lightning injury |
| Chemical burns |
| Inhalation injury |
| Burns in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality rateAny patients with burns and concomitant trauma (such as fractures) in which the burn injury poses the greatest risk of morbidity or death |
| Burn injury in children at hospitals without qualified personnel or equipment for the care of children |
| Burn injury in patients who will require special social, emotional or long-term rehabilitative intervention |
A severe burn patient will potentially suffer from hypovolemic shock, hypoxia, hypothermia and severe pain, all of which justify early advanced care, while management of the wound itself can initially remain for later.
Every second is precious and the quicker the first aid is provided the minimal is the extent of damage.10
Prehospital approach management to burn patient includes a safe approach and removing the victim from the source: hot and burned clothing and debris should be removed.
Initial management of chemical burns involves removing saturated clothing, brushing the skin if the agent is a powder, and irrigation with copious amounts of water, taking care not to spread chemical on burns to adjacent unburned areas. Irrigation with water should continue from the scene of the accident through emergency evaluation in the hospital. Efforts to neutralize chemicals are contraindicated due to the additional generation of heat, which would further contribute to tissue damage. A rescuer must be careful not to come in contact with the chemical, i.e., gloves, eye protectors, etc., should be worn. Removal of a victim from an electrical current is best accomplished by turning off the current and by using a nonconductor to separate the victim from the source.3
After extrication, initial care of burn victim is performed following the basic principles of any trauma resuscitation: ABCDE's (Advanced Trauma Life Support Guidelines).
Paramedics, other victims or the patient, can provide important information such as what burned, location of fire (enclosed or open space), explosion occurred (possibly causing a blast injury), whether the patient used alcohol or drugs and whether there was associated trauma.
History of previous diseases should be obtained, if possible (allergies, medications, past medical history, events).
It is mandatory to perform a rapid primary evaluation and immediately correct any problems found.
AirwayThe assessment must be made as to whether the airway is compromised or is at risk of compromise.11
In airway assessment, care provider should look for signs of inhalation injury (i.e., carbonaceous sputum, singed facial or nasal hairs, facial burns, oropharyngeal edema, vocal changes or altered mental status). If one or more of the signs of inhalation are present, administration humidified oxygen via a nonrebreathing reservoir mask or endotracheal tube will be placed and administrated 100% oxygen.
Inhalation of hot gases will result in burn above vocal cords. This burn will become oedematous over the following hours, especially after fluid resuscitation has begun.
If there is any concern about the patency of the airway then intubation is the safest policy.
However, an unnecessary intubation and sedation could worsen a patient's condition.11
Endotracheal intubation and mechanical ventilation are indicated when there is clinical evidence of respiratory failure, major inhalation injury or massive facial swelling or unconsciousness. Even then, in our experience when burn size exceeds 50% TBSA of deep burn including face and/or neck, endotracheal intubation does appear to be advisable.
Intubation itself is not without risk so it should not be undertaken routinely simply because there are facial burns.2 Flash burns often harm the face but rarely involve the airway, unlike severe burns from prolonged heat exposure associated with smoke inhalation.12
BreathingAll burns should receive 100% oxygen.
Several problems can compromise respiration in burn patients. When burn injury occurs in a closed space, carbon monoxide and cyanide poisoning must be suspected.13
CirculationFluid administration should begin immediately with lactated Ringer if transport time will be longer than 30min. The indications for fluid resuscitation include thermal injuries involving greater than 20% of TBSA and evidence of burn shock.14
Neurological disabilityAll patients should be assessed for responsiveness with the Glasgow Coma Scale (GCS). Considerer hypoxia or hypovolaemia and trauma associated.15
Exposure with environment control: initial dress woundThere is consensus in the recommendation that after a burn injury happens, cool running water should be applied immediately (12–15° is preferred),16 for 20–30min. There is not consensus about the time of effectiveness of this procedure after the injury. Some authors state that cool running water only has beneficial effects during the first hour17 while other authors declare that it is still effective until 3h, limiting tissue injury. When the burn lesion covers more than 10% of TBSA we must monitor the patient because of the risk of hypothermia, and warm him up if necessary.18 However it is essential to keep the patient warm.16
Neither direct application of ice, because it can cause new injuries, nor cold-water application is advised, as there is a risk of hypothermia. For emergency treatment or initial treatment at the place of injury, it is recommended to cover the wounds, when possible with sterile drapes.
When ventilatory and circulatory competence have been restored, a secondary survey should be performed to assess burn size and depth, to give analgesia to the patient, first wound care and establish referral indications to a Burns Unit (Table 2).11
Burn care in the Burn UnitSecondary survey is designed as a burn-specific evaluation. It is performed during admission to the burn unit and management of the wound should be performed. Full history should be approached including: detection of the mechanism of injury, consideration of abuse, height and weight, possibility of carbon monoxide intoxication, and facial burns.
Pan-CT and Fast-Echo should be performed when associated injuries are suspected.11
Assessment of burn area and depthTo calculate the extent of the burn, Wallace's “rule of nine” is a useful guide.
The adult body configuration is such that anatomical regions represent 9% of TBSA or a multiple thereof: head plus neck and each arm, 9%; anterior trunk, posterior trunk and each leg, 18%. In children, the relative body surface area of the head and neck is larger, and that of the lower extremities smaller than in adults.
A more precise age-adjusted estimate of relative body surface area in children can be made using the Lund and Browder.
A useful adjunct for calculating the size of partially burned areas of skin is the palm of the patient's hand which represents 0.5% of TBSA.
Assessing burn depth can be difficult. On direct examination, there are four elements that should be assessed. Bleeding on needle prick, sensation, appearance and blanching to pressure.
Burns are classified into two groups by the amount of skin loss. Partial thickness burns do not extend through all skin layers, whereas full thickness burns extend through all skin layers into the subcutaneous tissues.
Partial thickness can be divided into superficial (burn affects the epidermis), superficial dermal (burns extends through the epidermis into the upper layers) and deep dermal (burns extends through the epidermis into the deeper layers of the dermis but not through the entire dermis).
The degree of burns is calculated to estimate the prognosis, the amount of intravenous fluids (second and third degree) as well as the type of treatment and surgery that should be conducted.
Morbidity and mortality rises with increasing burned surface area. It also rises with increasing age so that even small burns may be fatal in elderly people.
PrognosisSurvival after burn has steadily improved over the last few decades. Patient mortality is, however, still the primary outcome measure for burn care. Scoring systems aim to use the most predictive premorbid and injury factors to yield an expected likelihood of death for a given patient.
The Baux rule is a simple scoring system based on predictor variables that are available without the use of laboratory tests or special instrumentation.
It is a simple rule of thumb to calculate the Burn Index (BI) that adds the age of the patient to the percentage of body surface area burned. This rule assumes that TBSA burns exceeding 75% indicate a poor prognosis.
The Abbreviate Burn Severity Index (ABSI) has an acceptable predictive value for mortality.19 This index is based on five variables: age, sex, presence of full-thickness burned, percentage of TBSA burned, and presence of inhalation injury. It is as simple and as easy to use as the clinical rule of thumb of Baux, yet it is more accurate and specific in describing outcomes for the victims of burn injury. This index, however, does not take into account preexisting diseases that have a significant influence on outcome. However, chronic alcohol abuse and smoking, inhalation injury, and pre-existing cardiac and neurologic conditions may have a significant impact in borderline groups with an ABSI score of 7–10.20 In spite of these questions, common burn severity scores are more discriminatory than the general APACHEII for severe burn patients.21
Smoke inhalation injuryDespite advances in ventilatory management, inhalation injury remains a leading cause of death in adult burn victims. The risk of inhalation injury increases with the extent of the burn and is present in two-thirds of patients with burns greater than 70% of TBSA.
The treatment of pulmonary parenchymal injury is inherently more complex than treatment for cutaneous burns. Necrotic skin can be excised, and healing can be observed directly. In contrast, injured lung involves measures to prevent further injury to allow host mechanisms to repair injured tissues. Healing of pulmonary injury is followed indirectly by observations of blood gas analysis and radiographs.
The term “smoke inhalation injury” refers to injury caused by inhalation of hot gaseous and toxic products of incomplete combustion. This syndrome is caused by three different entities:
- •
Upper airway thermal injury
- •
Chemical/inflammatory injury of the lower airways
- •
Systemic damage
It is important to obtain information on the source of the fire, the presence of smoke, duration of exposure, whether smoke inhalation occurred in a closed space, and the initial neurological condition of the patient.
The degree of respiratory injury is influenced by the extent of exposure, the toxicity of the smoke constituents to which the patient was exposed, the temperature, oxygen levels, concentration of smoke (air to fuel ratio) and systemic response secondary to inhalation, which could be responsible for tissue damage in the lungs.
Upper airway injuryUpper airway injury can be caused by direct thermal damage or chemical irritation. The inhalation of hot air at temperatures of 150°C and above will usually cause direct thermal injury to the face, oropharynx and upper airway. While heat and the chemicals in smoke cause immediate injury to the mucosa, the physiological consequences only become obvious once there is sufficient swelling to compromise the upper airway. The presence of skin burns in this region magnifies the problem in direct proportion to the extent and depth of the burn. The volume of fluids required when treating burn patients and mediators released following thermal injury both influence the extent of airway edema.
DiagnosisUpper airway involvement should be suspected in the event of smoke inhalation in closed spaces, burns to the face, neck, lips and oropharyngeal mucosa, singed nasal hairs and the presence of progressive hoarseness or a cough productive of carbonaceous sputum.
The clinical picture may progress to obstructive symptoms. Stridor, dyspnea, increased respiratory effort and cyanosis appear only once critical narrowing of the airway occurs. Stridor often precedes obstruction. Airway edema and swelling of burnt skin tissues follow a similar course, with internal and external anatomical distortion.
All burn patients should undergo inspection of the oropharynx for the presence of soot, or evidence of chemical or thermal damage. Direct laryngoscopy is a useful, quick and simple procedure. Immediate injury to the airway mucosa manifests itself by the presence of edema, erythema and ulceration. Due to the fact that edema may progress over 24h, multiple examinations are required if airway injury is confirmed and no intubation was performed. Fibroscopy may also be useful if airway damage is suspected and to assess known lung damage.
TreatmentIt is important to decide whether to protect the airway by endotracheal intubation or if it can safely be managed without this procedure. One should not wait for signs of obstruction to proceed with intubation. When in doubt of whether progressive edema is likely, it is safest to intubate. There are three categories of patients at risk for airway compromise.22
- (a)
Heat and smoke injury plus extensive facial and neck burns: this group invariably requires intubation.
- (b)
Significant oral burns but no smoke injury: these patients have difficulty controlling secretions as edema evolves. Early intubation is the safest approach, as anatomical distortion of the mouth may hinder the process at later stages.
- (c)
Heat and smoke injury, no facial burns: if there are no signs of severe upper airway edema, close monitoring may suffice.
Damage to the lower airways and lung parenchyma following smoke inhalation tends to be chemical rather than thermal. Toxic substances in smoke damage the epithelium and capillary endothelial cells of the airways: mucociliary transport is impaired and bacterial clearance reduced; inflammation, edema and bronchospasm may cause airway obstruction; the loss of surfactant facilitates alveolar collapse and atelectasis; in addition, increased capillary permeability magnifies pulmonary and airway edema.
Progressive respiratory damage may not be directly proportional to the degree of exposure to smoke. This is probably due to the composition of the inhaled material and differences in the host response.
DiagnosisSeverity is diagnosed based on the clinical course rather than initial findings.
Soot remains present in lung secretions for several days after injury. Roncus and wheezing appear at the onset of inflammation. Continuous cough, bronchospasm and bronchorrhoea can lead to fatigue and hypoventilation. The most serious clinical consequences are airway obstruction and bronchospasm, which usually start within the first 24h, and intrapulmonary shunting and pulmonary infection, which usually develop in the next few days.
The diagnosis of inhalation injury is clinical and accompanied by a set of indirect observations. While the presence of carbonaceous secretions is an indicator of exposure to smoke, it does not establish the diagnosis or the severity of inhalation injury. Chest X-rays lack the necessary sensitivity to detect lung damage in the early stages, but its use is helpful as a baseline for determining future changes. Chest CT can be used to complement bronchoscopy in detecting clinically significant inhalation injury.23
TreatmentPatients with smoke inhalation and burn injury require greater resuscitation volumes than patients with skin burns alone.
Adequate oxygenation must be maintained and bronchial hygiene facilitated. Some patients may receive non-invasive ventilation in the absence of usual contraindications.24 Endotracheal intubation may be necessary if the patient has increased work of breathing or if gas exchange is compromised. The consensus recommendations for mechanical ventilation also apply in this context, as do strategies for the prevention of ventilator-associated pneumonia (keep the head of the bed elevated, optimize endotracheal tube cuff pressure, adjust the patient's posture and perform mouth care). Prone positioning may be helpful in hypoxic patients. Bronchodilators may be administered to help optimize ventilation in the event of bronchospasm.22,24 Bronchoscopy can help improve pulmonary hygiene and patient prognosis by clearing secretions and sloughed epithelial cells.24
The effectiveness of aerosolised heparin is unclear. Inhaled nitric oxide (INO) causes selective vasodilation in well-ventilated lung segments, and may improve oxygenation and pulmonary hemodynamics. Antioxidants aerosols, cytokine inhibitors and neutrophil adherence inhibitors were tested in experimental studies, showing a reduction of mucosal and alveolar edema and atelectasis.
Extracorporeal membrane oxygenation (ECMO) is used as a rescue treatment in refractory situations and is not a standard therapeutic option at this time.
Systemic damage: carbon monoxide (CO) and cyanide poisoningWhile the gas-phase components of smoke produce no direct injury to the respiratory tract, they typically produce systemic effects.25
CO is an odorless, colorless gas produced by incomplete combustion of many materials. CO crosses the alveolar-capillary membrane, and causes tissue hypoxia via several mechanisms: (a) CO displaces oxygen from hemoglobin (Hb) as its binding affinity is 200 times higher; this decreases the arterial oxygen content (although oxygen pressure and saturation, i.e., PaO2 and SaO2 remain normal); (b) shifts the oxygen–Hb dissociation curve to the left, thus decreasing peripheral tissue O2 availability; (c) impairs mitochondrial function and ATP production; (d) CO can bind to skeletal and cardiac muscle where it produces toxic effects; it also causes central nervous system (CNS) demyelination.26
Cyanide is produced by the combustion of various nitrogen-containing materials, some natural, and some synthetic. Aerosolised and inhaled cyanide is rapidly absorbed in the lungs. It acts by binding to cytochrome oxidase, thereby inhibiting cell metabolism and tissue ATP production.26,27 All cells, in the liver especially, have the ability to detoxify cyanide through conversion to thiocyanate, which is then excreted in the urine. Large amounts of cyanide may cause this protection system to become saturated, especially if the patient happens to be hypovolaemic, thus impairing cyanide metabolism and clearance.
The combustion process also consumes oxygen, which decreases the fraction of inspired oxygen in the room. The combination of carbon monoxide and cyanide poisoning and breathing of oxygen-depleted air leads to tissue hypoxia.
DiagnosisThe clinical manifestations of CO poisoning appear when levels of carboxyhemoglobin (COHb) rise above 15%. The symptoms are typical of tissue hypoxia, most notably neurological impairment and myocardial dysfunction (the organ systems most vulnerable to hypoxia). There is no set combination of symptoms that confirms or rules out a diagnosis of CO poisoning. The intensity of clinical manifestations varies and does not correlate closely with COHb levels. Early signs tend to be neurological. CNS injury can lead to progressive and permanent damage. Severe myocardial dysfunction may occur, especially in patients with pre-existing coronary disease. The clinical diagnosis of CO poisoning should be confirmed by demonstrating elevated COHb levels. COHb can be measured by laboratory spectrophotometry of blood obtained at the scene and transported with the patient to the hospital, or obtained at the time of patient evaluation in the emergency department. Pulse CO-oximetry, where a probe is positioned on the fingertip is a technology which has been available since 2005. Although its accuracy and reliability have been reviewed, the results are somewhat controversial. As such, if pulse CO-oximetry supports the diagnosis, spectrophotometry measurements are recommended for confirmation. The determination of elevated COHb levels also indicates significant exposure to smoke, which points to the likelihood of chemical airway injury. Low COHb levels do not always mean minimal exposure, as oxygen management in the early stages can reduce levels during transport to the emergency department.
Cyanide poisoning has a similar clinical presentation, with metabolic acidosis and blurred vision in severe cases.28 The level of toxicity depends on the concentration of cyanide in the smoke. Persistent metabolic acidosis in a burn patient with adequate fluid resuscitation and cardiac output suggests carbon monoxide or cyanide poisoning. Acid–base balance and plasma lactate measurements are useful to determine intoxication. However, diagnosis is more difficult, as it is not possible to determine levels of cyanide (values below 0.1mg/L are considered normal).
Treatment“In situ” treatment is the same in both cases: remove the victim from the enclosure as soon as possible, and immediately administer high-flow oxygen.
The goal of oxygen therapy in patients with carbon monoxide poisoning is to displace CO from Hb. Levels of COHb decrease about 50% every 20min under administration of 100% oxygen. To successfully treat CO poisoning, it is important to know the concentration of COHb as soon as possible and administer oxygen therapy until levels of COHb fall below 10%.
Hyperbaric oxygen therapy (HBOT) (2–3atm) achieves faster CO displacement and is more useful in cases of prolonged exposure, when it is harder to displace CO from the cytochrome system. The drawback of HBOT is the need to transfer the burn patient to a treatment facility equipped with a hyperbaric chamber during the critical period of hemodynamic and pulmonary instability. It may be considered in patients with severe neurological involvement and levels of COHb greater than 50%, without extensive burns or severe lung damage, and whose symptoms fail to improve despite high-flow oxygen.22
Endotracheal intubation with 100% oxygen and mechanical ventilation is indicated in patients with severe neurological impairment and elevated COHb.
The management of cyanide poisoning focuses on cardiopulmonary optimization. This measure is usually sufficient, as the liver clears cyanide from the bloodstream.
Hydroxocobalamin should be given as early as possible in patients with possible smoke injury (traces of soot in the mouth, pharynx or sputum) who exhibit neurological impairment (confusion, coma, agitation, seizures) or one of the following: bradypnoea or respiratory/cardiac arrest; shock or hypotension; lactate ≥7.5mmol/L or metabolic acidosis. Dosage: 5g (2 vials) hydroxocobalamin administered as an intravenous (IV) infusion over 15min in adults; repeat dose (5g) if no improvement.22,29 The action of hydroxocobalamin in the treatment of cyanide poisoning is based on its ability to tightly bind to cyanide ions. Each hydroxocobalamin molecule can bind one cyanide ion by substituting it for the hydroxo ligand linked to the trivalent cobalt ion, to form cyanocobalamin. Cyanocobalamin is a stable, non-toxic compound which is excreted in the urine. Patients may show reversible red coloration of the skin and mucous membranes. Fairly marked, dark red chromaturia is normal in the 3 days following administration of the drug.
Amyl nitrite, sodium nitrite and sodium thiosulfate are helpful in cyanide poisoning when used individually, but a synergistic effect may occur with concomitant use. Nitrites induce methaemoglobinaemia which, together with carboxihemoglobinaemia may interfere with oxygen transport, thus contributing to hypoxia. Nitrites should therefore be used with caution in patients with smoke inhalation syndrome, and one should be reasonably sure of the diagnosis before administering these compounds.22,30,31 Sodium nitrite 3% is administered at doses of 300mg IV over 5–10min. High (or even recommended) sodium nitrite infusion rates may cause hypotension, so that vasopressor support may be required. Sodium thiosulfate acts as sulfhydryl group donor and promotes the conversion of cyanide to thiocyanate (which is less toxic). Dosage: 12.5g (50ml of 25% solution) over 10–15min, IV. Amyl nitrite is administered by inhalation at doses of 0.2–0.4ml. In the event of inadequate patient response, further doses of sodium nitrite and thiosulfate may be administered 30min later at half the initial dose.31
Initial management in non-thermal injuriesChemical burnsMore than 25,000 chemicals are used in the industry, agriculture, house cleaners and others and many of them have been identified as having the potential to cause burns.
The variety of chemical agents is so vast that it makes impossible to describe all treatments, but we can provide general principles for the management and treatment of chemical injuries.
Chemical burns only represent near the 3% of all burns but they present an important morbidity, commonly involve cosmetic body, like face, thorax and hands and in some series carry approximately a 30% mortality.32
PathophysiologyChemical injuries have some important biochemical differences when compared to thermal burns. In thermal injuries, there is a rapid coagulation of protein due to irreversible cross-linking reactions, whereas in chemical burns the protein destruction is continued by hydrolysis mechanisms. These mechanisms may continue so long as traces of the offending agent are present especially in deeper skin layers. In addition, chemical agents may produce a systemic toxicity.
The severity of a chemical burn injury is determined by: concentration of agent, quantity of burning agent, duration of skin contact, penetration power and mechanism of action.
Chemical injury is classified either by the mechanism of action or by chemical class of the agent.
Mechanisms of actionThere are six mechanisms of action for chemical agents in biological systems: Oxidation (sodium hypochlorite, potassium permanganate, chromic acid) reduction (hydrochloric acid, nitric acid) corrosion (phenols, sodium hypochlorite, white phosphorous), protoplasmic poisons (formic and acetic acids), vesicants (mustard gas) and desiccants (sulfuric and muriatic acids).
Type of chemicals:Acids: They release hydrogen ions and reduce pH from 7 to values as low as 0. Acids with a pH less than 2 can produce coagulation necrosis on contact with the skin.
Bases: Alkalis with a pH greater than 11.5 produce severe tissue damage through liquefaction necrosis. This tissue liquefaction allows deeper penetration of the agent. For this reason, alkali burns tend to be more severe than acid burns.
The ABC of Trauma, Primary and Secondary Assessment and all general principles of Trauma and Burn Care apply to chemical burns. However, there are also some measures of first aid that must be applied in chemical burns:
- -
Removal of the chemical agent and irrigation of burn area: the duration of the chemical's contact with skin is the major determinant of injury severity. This removal involved clothing and a thorough irrigation with water at the scene of accident. It should be repeated when patient arrives at Burn Center. Periods of 30min to 2h of lavage may be necessary to keep pH between 5 and 11. There are a few notable exceptions, because same chemicals produce significant exothermy when combined with water and also other chemicals are insoluble in water. These are the cases of dry lime, muriatic acid and concentrated sulfuric acid.
- -
Neutralizing agents: this is a controversial point. In most instances, antidotes should be avoided. Dilution, not neutralization, is the key to therapy. There are two notable exceptions: hydrofluoric acid (subeschar injection of 10% calcium gluconate until pain is relieved) and white phosphorous (lavage with 1% or 2% copper sulfate immerse in water).33,34
- -
General support and local care: conventional thermal burn formula for resuscitation is used with urine output monitoring to assessment of adequacy of end-organ perfusion. Disturbances of pH are the major systemic complications. Blood gas and electrolyte analysis should be performed until metabolic disorder has been treated.
On the other hand, clinical assessment of the deep and extent of a chemical burn is difficult because of the unusual skin tanning and anesthetic properties of same chemical agents. After lavage and debridement of blisters, chemical burns can be treated with similar local chemotherapeutic agents and dressings. Early excision and grafting should be planning as soon as possible.
Eyes are often involved in chemical burns. In these cases, immediate treatment with copious irrigation, prior to ophthalmic evaluation.35 Topical anesthetic drops may be applied to reduce the pain and to facilitate irrigation. According to the American National Standards Institute (Standard Z358.1-1990) severe eye burns have to be rinsed for 15min. At least 500–1000ml of irrigation is thus necessary. This intensive irrigation has a decisive influence on the clinical course and prognosis of such eyes.36
An anmphoteric solution for irrigation is Diphoterine (Previn®, Fa. Prevor). This synthesized fluid is able to bind both alkalis and acids, with a rapid reduction of pH in the conjunctival sac and in the corneal stroma.
Systemic toxicity: Burn team must be aware of any possible toxicity derived of systemic absorption of the chemical agent. Hydrofluoric acid toxicity includes hypocalcemia and ventricular fibrillation. Formic acid absorption can produce intravascular hemolysis, renal failure and pancreatitis. Liver dysfunction may appear also in hydrocarbures. Inhalation injury may occur in chemical burns when aerosolized chemical or smoke is inhaled. They are managed like smoke inhalation injuries.
In conclusion, patients must be treated by specialized burn team and referred to a Burn Center as soon as possible. The gold standard for treatment is still copious irrigation immediately after accident and prolonged in Burn Unit for maximal effect. Systemic toxicity and inhalation injury are rare but often severe and increase mortality.37
Special focus in chemical eye burn is necessary. First aid with intensive sterile irrigation with normal saline after injury has the greatest influence on prognosis and outcome. Irrigation should not be interrupted during transport to a Burn Unit.
Electric burnsElectrical injuries (excluding lightning) are responsible for >500 deaths per year in USA. A little more than half of them occur in the workplace and electrocutions at home account for >200 deaths per year and they are mostly associated with malfunctioning or misuse of consumer products. Electrical injuries are also the cause of considerable morbidity. Special important is the possibility of iatrogenic electrical injury in the ICU, or operating room, where several procedures are performed utilizing high-voltage energy for diagnostic and therapeutic purposes.38
PathophysiologyElectrical current exists in two forms, the alternating current (AC) and the direct current (DC). AC current is the most commonly used in households and offices, and it is standardized to a frequency of 60Hz. When the current is direct, the electrons flow only in one direction. This type of current is produced by various batteries and is used in certain medical equipment such as defibrillators, pacemakers, and electric scalpels. Although AC is considered to be a far more efficient energy, it is also more dangerous than DC (approx. three times) because it causes titanic muscle contractions that prolong the contact of the victim with the source. Lighting is a form of DC.
Burn electrical injury is caused by passage of current through the body (solid conductor) resulting in conversion of electrical energy to heat. In general, the type and extent of an electrical injury depends on the intensity of the electric current. Exposure of different parts of the body to the same voltage will generate a different current because resistance varies significantly between various tissues. The least resistance is found in nerves, blood, mucous membranes and muscles; the highest resistance is found in bones, fat and tendons. Skin has intermediate resistance.
The duration of the contact with electrical current is an important determinant of injury. In the same way, the pathway of the current through the body, from the entry to the exit point, determines the number of organs that are affected and, as a result, the type and severity of the injury. A vertical pathway parallel to the axis of the body is the most dangerous because it involves virtually all the vital organs (central nervous system, heart, respiratory muscles and in pregnant women, the uterus and the fetus). A horizontal pathway through the lower part of body may cause severe local damage but will probably not be lethal.39,40
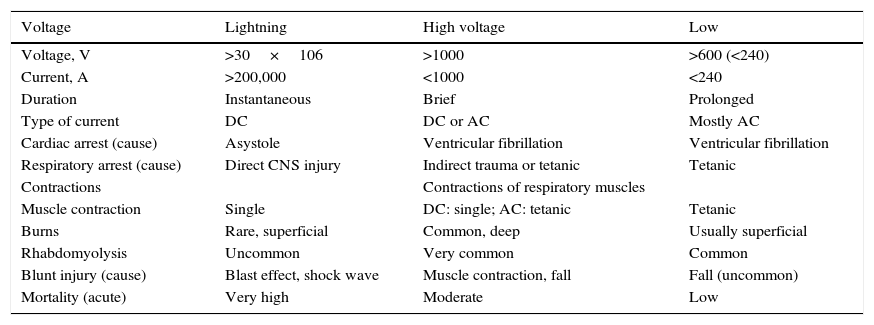
Electric shock from a low-voltage line is delivered on contact of the victim with the source, and in high-voltage injury, the current is carried from the source to the person though an arc before any actual physical contact is made. Arcs can generate extremely high temperatures (up to 5000°C) that are usually responsible for the severe thermal injuries from high voltage (Table 3).
Comparison between lightning, high-voltage, and low-voltage electrical injuries (based on data obtained from reference38).
| Voltage | Lightning | High voltage | Low |
|---|---|---|---|
| Voltage, V | >30×106 | >1000 | >600 (<240) |
| Current, A | >200,000 | <1000 | <240 |
| Duration | Instantaneous | Brief | Prolonged |
| Type of current | DC | DC or AC | Mostly AC |
| Cardiac arrest (cause) | Asystole | Ventricular fibrillation | Ventricular fibrillation |
| Respiratory arrest (cause) | Direct CNS injury | Indirect trauma or tetanic | Tetanic |
| Contractions | Contractions of respiratory muscles | ||
| Muscle contraction | Single | DC: single; AC: tetanic | Tetanic |
| Burns | Rare, superficial | Common, deep | Usually superficial |
| Rhabdomyolysis | Uncommon | Very common | Common |
| Blunt injury (cause) | Blast effect, shock wave | Muscle contraction, fall | Fall (uncommon) |
| Mortality (acute) | Very high | Moderate | Low |
Electrical injury should be managed as a multisystem injury. Although multisystem injuries can be very extensive, it is damage to the vital organs that may require intensive care.
The most potential injuries are as follows:
- –
Cardiovascular system
Pathophysiology. Electrical injury may affect the heart in two ways: by causing direct necrosis of the myocardium and by causing cardiac dysrhythmias. To same extent, the degree of myocardial injury depends of the voltage and the type of current, being more extensive with higher voltage and more severe with AC than DC electrical current.41
Injury usually consists of widespread discrete, patchy contraction band necrosis involving the myocardium, nodal tissue, conduction pathways and the coronary arteries. Rhythm disturbances may be produced with exposure to relatively low currents. A current of more than 50–100mA with hand -to-hand or hand-to-foot transmission can cause ventricular fibrillation. Exposure to high-voltage current will most likely cause ventricular asystole. Lightning acts a massive cosmic countershock that causes cardiac standstill.
Late dysrhythmias are probably due to arrhythmogenic foci secondary to patchy myocardial necrosis and especially due to injury of the SA node.
Clinical manifestations. Cardiac standstill and ventricular fibrillation are the most serious of the cardiac complications of the electric injury. However, there are also several other dysrhythmias with better prognosis. Nonspecific ST-T changes are the most common ECG abnormality and atrial fibrillation is the most common dysrhythmia.42
- –
Cutaneous injuries
Pathophysiology. Exposure to currents generated by low-voltage sources may cause a variety of cutaneous injuries from the transformation of electrical to thermal energy. The injuries can range from the transformation of electrical to thermal energy. The injuries can range from local erythema to full-thickness burns. The severity of the burns depends on the intensity of the current, the surface area and the duration of exposure.
The resistance of the skin may be markedly altered by moisture, and electric current may be transmitted to deeper tissues before it causes significant damage to the skin. Thus, in contrast with thermal burns, the severity of the skin burns cannot be used to assess the degree of internal injury in an electrical accident with low voltage.
More serious burns are usually caused by exposure to arcs that are created in accidents with high-voltage currents.
Clinical manifestations. They will depend on their extent and severity. When extensive flash and flame burns are present the patient is expected to develop severe hemodynamic, autonomic, cardiopulmonary, renal, metabolic and neuroendocrine responses.
- –
Nervous system
Pathophysiology. Usually nervous system injury is not due to the direct effect of the electrical current itself but due to trauma or dysfunction of other organ systems.
The passage of electrical current through the brain can cause injury to the respiratory control center that results in respiratory arrest. Acute cranial nerve deficits and seizures may also occur after electric injury to the brain. Direct injury to the spinal cord with transaction at the C4–C8 level may occur with a hand-to-hand flow. The most common indirect injuries causing significant central nervous system are brain ischemia or anoxia secondary to cardiorespiratory arrest and traumatic or spinal cord injury secondary to a fall. Peripheral nerves may incur secondary damage due to local burns or entrapment from scar formation, vascular injury or edema. Upper-motor neuro-deficits are common.
Clinical manifestations. Loss of consciousness, confusion and impaired recall tend to be very common among victims of electrical injury. Transient paralysis (keraunoparalysis) and peripheral vasospasm have been described in the context of electrical injury due to lightning.40
- –
Respiratory system
Pathophysiology. Although respiratory arrest is one of the common causes of acute death in severe electrical injury, there are no specific pulmonary injuries attributable to electric current.
Clinical manifestations. In addition to apnea in cases of respiratory arrest, patients may exhibit a variety of nonspecific respiratory patterns that reflect disturbances of other organ systems rather than from specific injury to the respiratory system.
- –
Other systems. Among other systems that may incur damage due to electrical injury, the kidneys are of particular importance. The kidneys are very susceptible to anoxic/ischemic injury that accompanies several electric injury. In addition, vascular compromise and muscle necrosis may cause renal tubular damage, leading to renal failure from release of myoglobin and creatinine phosphokinase.
Even then, skeletal system may have fractures either from severe muscle contractions or from injury due to falls from significant heights.
The eyes and the ears may be entry points of lightning strike and present a number of clinical problems. Transient autonomic disorders may cause fixed pupils after a lightning injury that in association an often unconscious patient, may be perceived as severe brain injury. Up to 50% of patients may experience rupture of the tympanic membranes and temporary hearing loss. Cataracts are a very common complication of lightning injury but rare acutely present.43
General management and prognosisThe management of severe electrical injuries requires a combination of cardiopulmonary resuscitation and acute multiple trauma care. Treatment may follow the same principles of resuscitation as any other traumatic injury.
In contrast with another traumatic injuries, in electrical injuries require special consideration the access to the victim giving the same threat to the rescuer as it does to the victim because, if the victim is still in contact with the source of the current he or she becomes a conductor that may electrocute the rescuer. Thus, no attempt to provide medical care should be made until either the source of the electrical current has been cut off or the victim has been extricated safely away from the current source.
Specifically for patients admitted to the ICU, the following issues should be considered:
- •
Evaluation for hidden injury (spinal cord injury) and for blunt thoracic or abdominal trauma.
- •
Serial evaluation of liver, pancreatic and renal function for traumatic and anoxic/ischemic injury with CT scan or ECO if considered.
- •
CT cerebral scan is indicated in severe cases of lightning injury, injuries due to a fall and there are abnormal neurologic findings.
- •
Evaluation of rhabdomyolysis and myoglobinuria. May be considered the administration of bicarbonate at 1–2mEq/kg to treat the underlying acidosis and alkalinizes the urine, making myoglobin more soluble and manitol 1g/kg to promote an osmotic dieresis.
- •
Evaluation of the limbs for compartment syndrome that requires urgent fasciotomy.
- •
Fasciotomy also serves a diagnostic role to determine the extent of muscular necrosis.
- •
Ophthalmologic and otoscopic evaluation.
- •
Fluid management. The combination of extensive burns and significant internal visceral injury leads to increased fluid requirements due to fluid extravasation into third space compartments and to ongoing fluid losses. High tension electrical injury requires substantially more fluid (up to 9ml×%TSBA×body weight) in the first 24h and a higher urine output (1.5–2ml/kg/h).
- •
Cardiac monitoring recommended: continuous telemetry, serial ECGs and serial measurements of cardiac enzymes CK-MB and Troponin T. CK-MB isoenzymes are not reliable indicators of cardiac injury after electrical burns and should not be used in decisions regarding patient disposition and insufficient data exists on troponin levels to formulate a guideline.
The prognosis depends on the severity of the initial injury and the development of complications. Due to the complexity of the problem, patients are at risk of developing multisystem organ failure that carries high mortality and even higher morbidity.
Since most electrical injuries are preventable, education and adherence to safety measures both at home and al work constitute the most important aspect of management.42
Conflict of interestNone
DisclosureNothing to disclose.

