






Today there is growing concern about the use of opiates. It is estimated that almost 40% of non-hospitalized US citizens received, at least, 1 opiate prescription in 2015.1 Although in Spain the problem does not reach such dimensions, interest has grown in an attempt to look for other alternatives to these drugs.
Although this is a shared concerned of intensive care units, the problem is more complex. Due to the patients’ characteristics, many of them with complex diseases, multiorgan dysfunction or large distribution volumes, analgesia without the use of opiates is certainly challenging.2 To this date and because of the COVID-19 pandemic, the problem has gained momentum. The hospitalization of a huge number of patients with severe respiratory distress requiring deep sedation for long periods of time and great opiate consumption is an added difficulty not only for their withdrawal, but also for the use of multimodal analgesia.
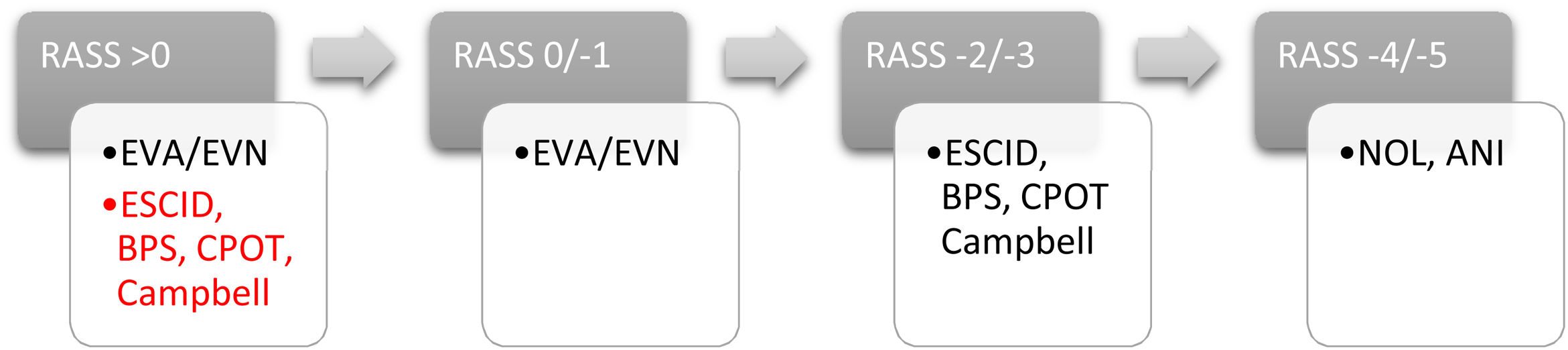
Based on the data published by Spanish intensive care units3 (ICUs), 29% of the patients admitted are prescribed opiates, a number that goes up to 70% in patients on invasive mechanical ventilation. However, only little over 52% of all IUCs use pain assessment scales in their routine clinical practice, a number that is much lower compared to the standards recommended. Therefore, if pain is to be approached appropriately, it is essential to perform assessments with specific scales designed for that purpose, both for communicative and non-communicative patients (Fig. 1), and consider individual therapies with multimodal analgesia strategies as the basis of treatment (Table 1).
Non-opiate analgesics for multimodal analgesia.
| Analgesic | Dosage | Specifics | Side effects |
|---|---|---|---|
| Paracetamol | 1 g IV/OR every 6−8 h | Avoid in liver failure. Metabolism through p450. | Hypotension, nausea, vomiting, headaches, liver damage. |
| Metamizole | 2 g IV every 6−8 h | Rate of agranulocytosis: <10 cases/million | Agranulocytosis, glottis edema, anaphylactic shock |
| 575 mg OR every 6−8 h | |||
| Dexmedetomidine | 0.2−0.8 μg/kg/h IV | α-2 Agonist | Bradycardia, arterial hypotension |
| Maximum 1.4 mcg/kg/h | |||
| Ketamine | IV pattern: | Non-competitive NMDA receptor antagonist | Rarely used at analgesic doses: daydreaming, hallucinations, and dissociative effects. |
| Bolus: 0.125–0.25 mg/kg | Uncommon psychomimetic effects used at analgesic doses | Arterial hypertension | |
| Infusion: 0.1–0.3 mg/kg/h | Useful in opiate-associated hyperalgesia | Tachycardia | |
| guideline SCR: | |||
| 0.1−0.5 mg/kg/h | |||
| Ibuprofen | 400 mg/6 h | Not considered a first-line drug at the ICU setting. | GI bleeding, ulcerations, bleeding, renal failure. |
| Ketorolac | 10 mg/IV/6 h | Not considered a first-line drug at the ICU setting. | GI bleeding, ulcerations, bleeding, renal failure |
| Dexketoprofen | 50 mg/IV/8−12 h. | Would be indicated for patients with pain of inflammatory characteristics (polytraumatized) | GI bleeding, ulcerations, bleeding, renal failure. |
| Lidocaine | IV pattern: | Calcium channel blockers | Agitation, tinnitus, metallic taste, seizures, coma, arrhythmias, cardiorespiratory arrest. |
| Bolus: 1.5 mg/kg | |||
| Infusion: 1−2 mg/kg/h | |||
| Magnesium | Single dose (prevention): | Non-competitive antagonist of NMDA receptor. Reduces the necessary dose of opiates | |
| 30−50 mg/kg/IV. | |||
| Continuous IV pattern: | |||
| Bolus: 50 mg/kg | |||
| Infusion: 10–25 mg/kg/h | |||
| Gabapentin | 1200–3600 mg/day OR distributed in 2−3 doses | Union to voltage-gated Ca2+ channels. Useful to treat neuropathic pain. | Slow action onset. Progressive dose titration. |
| Vertigo, sleeplessness, confusion, edema | |||
| Pregabalin | 300–600 mg/day OR distributed in 2−3 doses | Union to voltage-gated Ca2+ channels. Useful to treat neuropathic pain. | Slow action onset. Progressive dose titration. |
| Vertigo, sleeplessness, dry mouth, blurry vision, edema. |
If the current recommendations are followed, both the Pain, Analgesia, Delirium, Immobility and Sleep (PADIS) clinical practice guidelines published by the American Society in 20182 and those published in 2019 by the Pan-American Society,4 opiates should be considered the basis of analgesia in critically ill patients. However, both guidelines stress out the importance of the side effects opiates have, and the fact that critically ill patients can develop severe problems (ileus, respiratory depression, delirium, immunosuppression), which increases the morbidity and mortality rates and extends the ICU stay. In both publications, the lowest possible dose to achieve the desired therapeutic target for the shortest amount of time possible is advised. For this purpose, it is essential to perform routine monitoring of pain while using the proper scales.
Multimodal analgesia includes the use of a combination of analgesic drugs with different action mechanisms, and the application of different locoregional anesthetic techniques in the search for optimal analgesia using the lowest possible drug dose and, therefore, minimizing side effects. However, this is a complex approach in critically ill patients because the disease that eventually leads to the patient’s admission often includes, at least, single-organ dysfunction. Also, because of the pharmacological interactions that can occur among the different analgesics eventually leading to limitations in their use.5 In any case, it is evident that proper pain management is challenging in critically ill patients requiring a rigorous assessment of pain and the use of combined analgesics to minimize the use of opiates as much as possible.6 Although in the critically ill patient, the first choice is opiates, multimodal analgesia can be started to reduce the dose of opiates administered and prevent any side effects. Also, it is a feasible option for stable patients with mild-to-moderate pain upon admission to our units.
Instead of widely used analgesics (paracetamol, metamizole or NSAIDs), other less common drugs can be used. In the case of drugs like dexmedetomidine, ketamine, lidocaine or magnesium, although clinical experience on their use as analgesics in critically ill patients is still scarce, they can be useful to control postoperative pain, especially as part of a strategy of the opioid-free-anesthesia kind.5 Pregabalin end gabapentin are 2 drugs that should be taken into consideration for the management of neuropathic pain or hard-to-control headaches like those associated with subarachnoid hemorrhages while taking into account that according to their pharmacodynamic profile it can take days for their effects to appear.
Finally, regarding locoregional anesthetic techniques, paravertebral block and epidural analgesia are essential and they can be tremendously useful in postoperative or polytraumatized patients allowing a clear reduction of the use and dosage of analgesic drugs.7
However, one of the great challenges of analgesia in Intensive Medicine Services is chronic critically ill patients, who are those with prolonged stays and pain that is not only associated with the reason for admission, but also with procedures, manipulations and mobilizations, where the use and abuse of analgesics can be a real problem requiring a rotation of these drugs to avoid possible side effects associated with their continued use over time.8 In these patients, methadone is emerging as a drug to be considered due to its analgesic properties and as a strategy to withdraw from other opiates. Therefore, it is a drug that should be take into consideration (Table 2). It would be an important drug for patients with long opiate treatments within an opiate-withdrawal therapy.
Alternative opioids.
| Opiate | General characteristics | Orientative dosing |
|---|---|---|
| Remifentanil | 100 times more powerful than morphine. | IV analgesic dose: .5–3 μg/kg/h |
| Quick onset and end of action (<5 min). | IV sedative dose: 3–12 μg/kg/h | |
| Metabolized by plasmatic esterases. Does not accumulate in kidney and/or liver failure. | ||
| Its quick end of action can lead to pain/deprivation phenomena so the administration of a longer half-life opiate is advised prior to its withdrawal. | ||
| Avoid its administration in bolus (respiratory depression). | ||
| Fentanyl | 100 times more powerful than morphine. | IV bolus: 30–150 μg |
| Onset of action: 1–3 min. | IV perfusion: 30–150 μg/h | |
| Half-life: 30–60 min. Very lipophilic drug. Its administration through continuous infusion prolongs its half-life. | ||
| Of choice for the management of acute pain control in patients on spontaneous ventilation. | ||
| Liver metabolism leading to inactive metabolites. Adjust dose in liver failure. Does not accumulate in kidney failure. | ||
| Morphine | Onset and peak of action later than the previous ones. | IV bolus: 0.05–0.1 mg/kg |
| Half-life: 4–6 h. It is the best opiate for intermittent guidelines. | IV perfusion: 0.5–7 mg/h | |
| Liver metabolism leading to active metabolites that are eliminated through the kidney. To be avoided in cases of kidney failure. | ||
| It is associated with histamine release so it should be used with caution in patients with hemodynamic instability. | ||
| Methadone | Triple analgesic action: | Oral/enteral dose: 0.1–0.4 mg/kg administered every 8−12 h depending on response. |
| Mu-opioid receptor agonist. | ||
| NMDA receptor antagonist. | ||
| Serotonin and noradrenalin reuptake inhibitors | ||
| It takes days to reach stable concentration. Initially its administration is advised together with another opiate. | ||
| Assess its use in: | ||
| Patients requiring high doses of opiates. | ||
| Patients with pain that can be persistent in time. | ||
| Chronic opiate consumers. | ||
| Liver metabolism leading to inactive metabolites. | ||
| Avoid its administration in liver failure. | ||
| Avoid its administration with serotonin and noradrenalin reuptake inhibitors and those that prolong the QTc interval. | ||
| Tramadol | Double analgesic action: | Enteral/parenteral dose: |
| Mu-opioid receptor agonist. | 50−100 mg/6−8 h | |
| Inhibits reuptake of noradrenalin and serotonin. | ||
| Liver metabolism in first stage by O-demethylation to active metabolites. Dose should be considered in case of liver failure. Urinary excretion. | ||
| It has important side effects that limit its use: | ||
| Serotoninergic syndrome. | ||
| pro-seizure activity. | ||
| It has important drug interactions. | ||
| Sudden withdrawal of drug should be avoided. |
Both the assessment of pain and the administration of proper analgesia should be a priority in the management of critically ill patients. In the words of Chamorro et al., the administration of the right analgesia should not be an unfinished business for the intensivist, but part of the routine clinical practice.9 The appearance of signs of chronic pain after patients have been admitted to the intensive care unit recently included within the Post-ICU Syndrome is associated with a lower quality of life and delays coming back to activities of daily life, which is why they should be avoided.10 The use of a multimodal analgesia strategy to minimize opiate use, looking to diminish the side effects of this drug group and future dependencies, should be combined with proper monitoring to ensure good analgesia practices. This is the only way to be prevent pain from becoming one of the most unpleasant and long-lasting memories after the patients have been admitted to the intensive care unit and to return critically ill patients to a good-quality life.
Please cite this article as: García Sánchez M, Alcántara Carmona S. ¿Es realmente posible la reducción del uso de opiáceos en el paciente crítico? Med Intensiva. 2022;46:269–272.

