
Study and Evaluation of Two Scores: Shock Index (SI) and Physiological Stress Index (PSI) as discriminators for proactive treatment (reperfusion before decompensated shock) in a population of intermediate-high risk pulmonary embolism (PE).
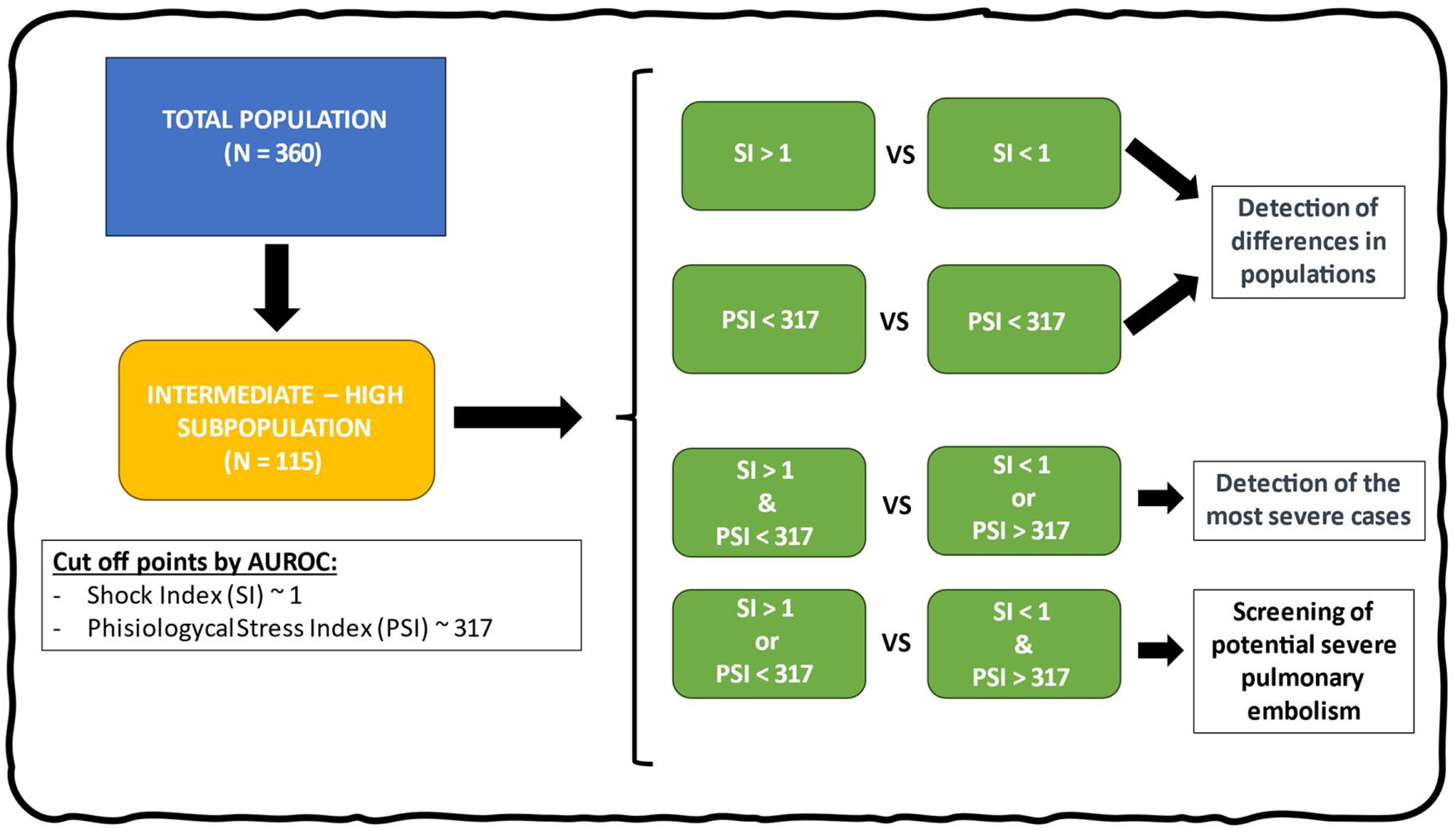
DesignUsing a database from a retrospective cohort with clinical variables and the outcome variable of “proactive treatment”, a comparison of the populations was conducted. Optimal cut-off for “proactive treatment” points were obtained according to the SI and PSI. Comparisons were carried out based on the cut-off points of both indices.
SettingPatients admitted to a mixed ICU for PE.
ParticipantsPatients >18 years old admitted to the ICU with intermediate-high risk PE recruited from January 2015 to October 2022.
InterventionsNone.
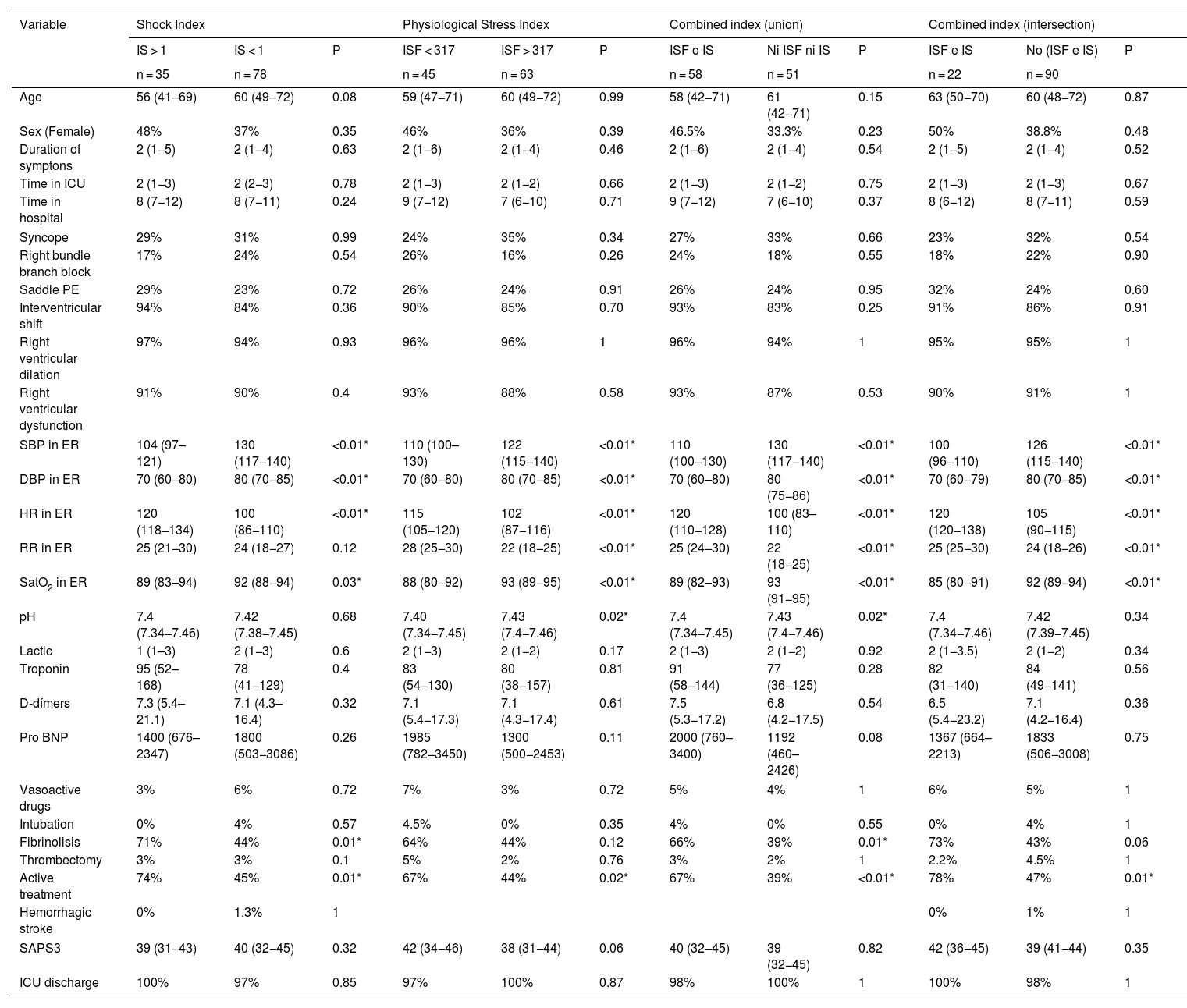
Main variables of interestPopulation comparison and metrics regarding predictive capacity when determining proactive treatment.
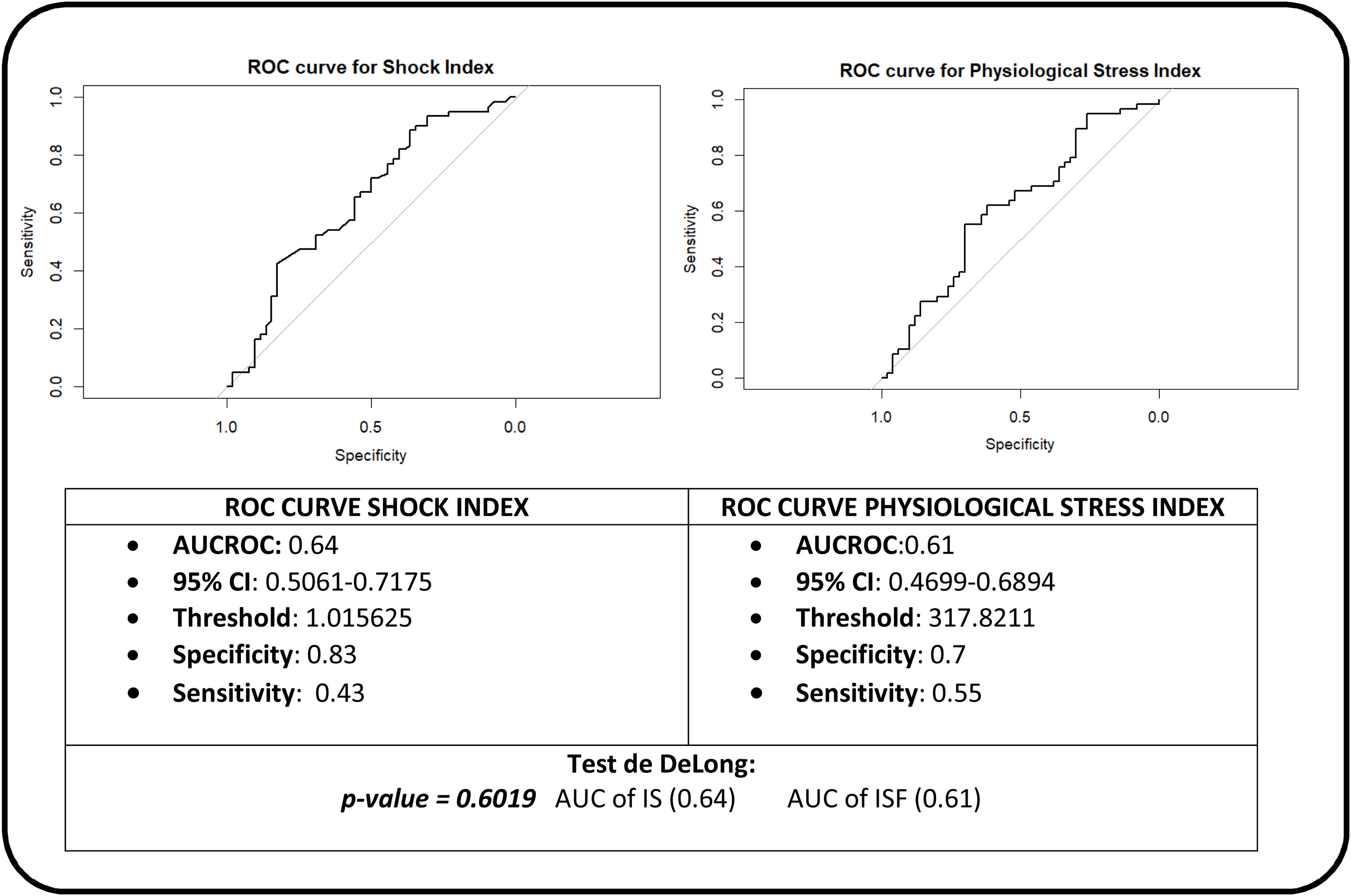
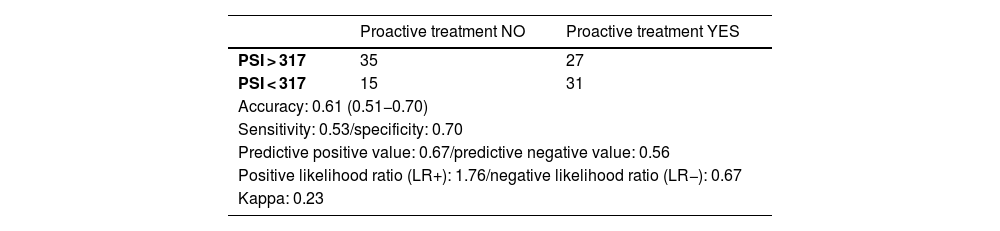
ResultsSI and PSI independently have a substandard predictive capacity for discriminating patients who may benefit from an early reperfusion therapy. However, their combined use improves detection of sicker intermediate-high risk PE patients (Sensitivity = 0.66) in whom an early reperfusion therapy may improve outcomes (Specificity = 0.9).
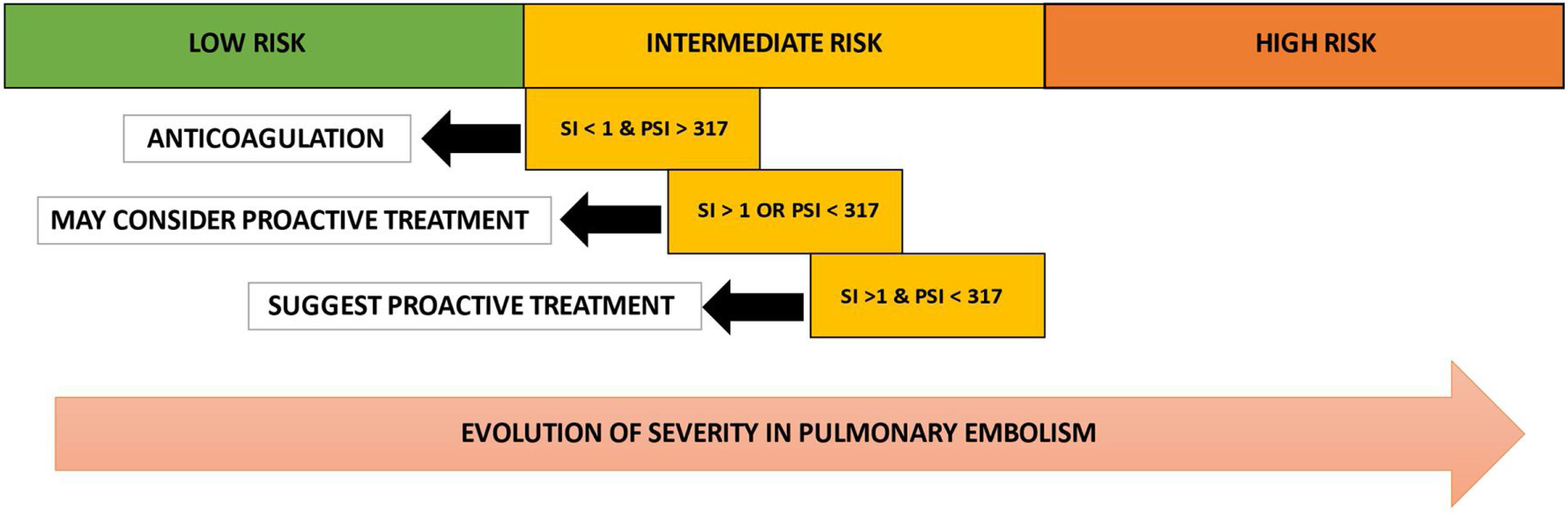
ConclusionsThe use of the SI and PSI in patients with intermediate-high risk PE could be useful for selecting patients who would benefit from proactive treatment.
Valoración de dos scores: Shock Index (SI) y Physiological Stress Index (PSI) como discriminantes de haber recibido tratamiento proactivo (Fibrinolisis o trombectomía) en una población de tromboembolismo pulmonar (TEP) de riesgo intermedio – alto.
DiseñoSobre una base de datos de una cohorte retrospectiva con variables clínicas se estudió la variable resultado “tratamiento proactivo” en función de los scores SI y PSI. Se obtuvieron los puntos de corte óptimos de haber recibido tratamiento proactivo según el SI y el PSI. Se realizaron comparaciones en función de los puntos de corte de ambos índices.
ÁmbitoPacientes que son ingresados en UCI mixta por TEP.
PacientesPacientes >18 años ingresados en UCI por TEP de riesgo intermedio-alto. Desde enero de 2015 hasta octubre de 2022.
IntervencionesNinguna.
Variables de interés principalesComparación poblacional y métricas en relación a la capacidad predictiva de los scores cuando se determina tratamiento proactivo.
ResultadosLos predictores SI y PSI tienen una capacidad predictiva regular para discriminar los pacientes sometidos a tratamientos proactivos de reperfusión. Su uso combinado mejoran la capacidad de detección de los pacientes más graves (Sensibilidad = 0.66) y que podrían requerir tratamiento (Especificidad = 0.9).
ConclusionesEl uso del SI y del PSI en los pacientes con TEP de riesgo intermedio-alto puede ser útil para seleccionar a pacientes que se beneficiarían de tratamiento proactivo.
Article
Go to the members area of the website of the SEMICYUC (www.semicyuc.org )and click the link to the magazine.


