




Immunotherapy seeks to harness the power of the immune system to eradicate malignant tissues. Despite impressive therapeutic success, however, it can be accompanied by severe adverse effects such as cytokine release syndrome (CRS). These therapies cause the release of a great amount of cytokines, with IL-6 playing a central role, that can potentially lead to multiple organ dysfunction. The diagnosis is based on the presence of compatible clinical symptoms, elevated biomarkers and recent treatment with a biological agent. Mild cases can be managed through symptomatic treatment and fluids, while more severe episodes may need supportive therapy and specific care with the anti-IL-6 receptor monoclonal antibody tocilizumab. Although corticosteroids are also effective, they suppress T-cell activity, and so should only be considered as second line therapy or in cases of severe neurological involvement, since tocilizumab does not cross the blood-brain barrier. Cytokine release syndrome generally has a good prognosis, often being reversible and with a good response to specific treatment. Despite possible concerns about the admission of such patients (mainly with advanced oncological disease), we consider that the Intensive Care Unit should remain an option, since these individuals present a potentially reversible drug-related adverse event and are being treated with a new drug that could change the prognosis of the disorder. Intensive care medicine will become a key component in the management of the complications of modern cancer therapies, dealing with patients presenting an overactive immune system producing organ dysfunction while also trying to maintain treatment efficacy. This is the new paradigm.
La inmunoterapia potencia el sistema inmunitario para erradicar las células malignas. A pesar de mostrar un importante éxito terapéutico, puede ir acompañada de efectos adversos graves, como el síndrome de liberación de citocinas. Dichas terapias pueden causar la liberación de importantes cantidades de citocinas, siendo IL-6 el mediador principal, e inducir un cuadro de disfunción multiorgánica. El diagnóstico se basa en la presencia de síntomas clínicos compatibles, elevación de biomarcadores y tratamiento reciente con un agente biológico. Los casos leves se pueden manejar con tratamiento sintomático y fluidoterapia, mientras que los episodios graves necesitarán tratamiento de soporte y específico con tocilizumab, un anticuerpo monoclonal anti-receptor de IL-6. Los corticoides, aunque efectivos, suprimen la actividad de las células T, por lo que su uso se considera de segunda línea o en afectación neurológica grave, ya que tocilizumab no cruza la barrera hematoencefálica. A pesar de que puedan existir dudas sobre el ingreso en unidades de críticos de estos pacientes, principalmente con enfermedad avanzada, consideramos que podrían beneficiarse del ingreso en las UCI, ya que se trata de pacientes con un evento adverso potencialmente reversible, recibiendo un nuevo fármaco que podría cambiar el pronóstico de su enfermedad. La medicina intensiva es clave en el manejo de las complicaciones de las nuevas terapias oncológicas, tratando pacientes con un sistema inmunitario excesivamente activado mientras se intenta preservar la eficacia del tratamiento. Este es el nuevo paradigma.
Cancer is a mayor public health problem worldwide, expected to become the leading cause of death in many developed countries.1 In Spain, it is the first cause of death in men and women over forty years, being responsible of 25% of global mortality.2 During the last two decades, mortality has significantly dropped by means of more effective therapies, including immunotherapy, and improvement in supportive therapy,3 reaching a 5 year survival around 50%.2
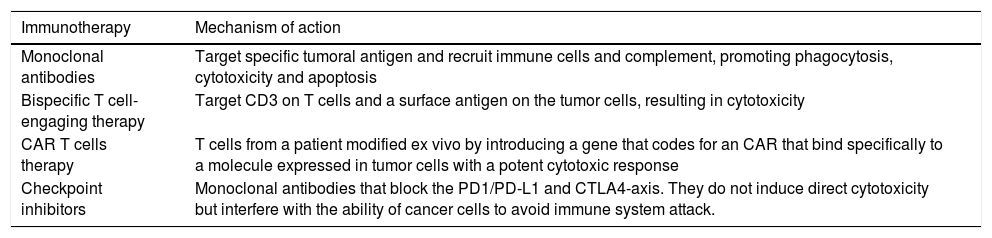
Immunotherapy is a type of biological therapy 4 that seeks to harness the power of the immune system to eradicate malignant tissues,5 while classic chemotherapy work by stopping or slowing the growth of cancer cells,6 which is associated with immunosuppression and infection.7 These new therapies include monoclonal antibodies (MAb), bispecific T-cell engaging (BiTe) therapy,8 checkpoint inhibitors 7 and cellular therapies, as chimeric antigen receptor (CAR) T-cells 9 and T-infiltrating lymphocytes (TIL) (Table 1). Despite showing impressive therapeutic success,10 these therapies are also accompanied by severe and life-threatening adverse effects, as severe cytokine release syndrome (CRS) and autoimmunity.11 CRS occurs as a result of massive release of cytokines after immunotherapy, while autoimmune occurs when the targeted tumor associated antigen is expressed on non malignant tissue, so-called “on target, off-tumor toxicity”.5 CRS occurs mainly after BiTe and CAR T-cell therapy, with a quite variable incidence, ranging from 2% to 94%, reflecting different prophylactic approaches, variable doses, underreporting and variable CRS definitions.10,12,13 Checkpoint inhibitors despite occasionally related to CRS14 are mainly associated with autoimmune events.7 Isolated cases of CRS have been related to hematopoietic stem cell transplantation (HSCT),15 and even conventional chemotherapy 11 and radiotherapy.16
Immunotherapy for cancer.
| Immunotherapy | Mechanism of action |
|---|---|
| Monoclonal antibodies | Target specific tumoral antigen and recruit immune cells and complement, promoting phagocytosis, cytotoxicity and apoptosis |
| Bispecific T cell-engaging therapy | Target CD3 on T cells and a surface antigen on the tumor cells, resulting in cytotoxicity |
| CAR T cells therapy | T cells from a patient modified ex vivo by introducing a gene that codes for an CAR that bind specifically to a molecule expressed in tumor cells with a potent cytotoxic response |
| Checkpoint inhibitors | Monoclonal antibodies that block the PD1/PD-L1 and CTLA4-axis. They do not induce direct cytotoxicity but interfere with the ability of cancer cells to avoid immune system attack. |
CRS was first described in 1989, in kidney transplant recipients treated with the anti-CD3 monoclonal antibody OKT3, which typically developed a flu-like syndrome one hour after the first infusion.17 The syndrome became more relevant after 1997, with the approval of rituximab and a myriad of MAb for the treatment of different cancers, many of them also related to the presence of CRS.18,19 Later on, in 2006, a severe CRS (sCRS) was induced in 6 healthy volunteers who received an anti CD28 monoclonal antibody (TGN1412), requiring ICU admission for respiratory distress and renal failure.20 In recent years, with the appearance of BiTe and cellular therapies, CRS has been increasingly reported.11
Over the last two decades, the number of cancer patients requiring ICU care has dramatically increased, with 15% of ICU beds occupied by cancer patients.3 With the extensive use of immunotherapy in cancer, CRS is being increasingly reported.7
Thus, intensive care medicine will become a key component in the management of the complications of modern cancer therapies.11 We will need to face patients with an over-active immune system, inducing severe organ dysfunction, while we try to keep the efficacy of the treatment. That is the new paradigm.
MethodsWe performed a review searching In Medline (Pubmed) database using the term “cytokine release syndrome” restricted to articles with the selected term present in title or abstract [TiAb]. All articles identified by the search were initially screened for eligibility on title and abstract independently by two reviewers. The references of the selected articles were in turn used to identify additional studies. Any differences were resolved by consensus.
PathophysiologyThe rising stars in cancer treatment (MAb, BiTe, CAR T-cell) are approaches by which the patient́s immunological self-defense is strengthened in a feasible and effective manner,7 enhancing the power of the immune system to destroy cancer cells,5 which can cause an excessive release of inflammatory cytokines,21 leading to a severe systemic inflammatory response and multiple organ dysfunction.22 The source of cytokines can be either target cells themselves or immune cells that have been recruited to the tumor site.11
All these therapies, in different ways, cause a significant activation of the immune system,10 including lymphocytes (B cells, T cells and/or natural killer cells) and/or myeloid cells (macrophages, dendritic cells, and monocytes) which lead to release of lymphocyte derived (IFN gamma, IL-6, sIL-2R alpha, sIL-6R, and GM-CSF) and monocyte/macrophage (IL1-receptor antagonist, IL-10, IL-6, IP-10, monokine, IFN alpha, MIP-1 alpha, MIP-1 beta, and sIL6R) cytokines.21 IL-6 plays a central role in CRS.5 There is also evidence of vascular endothelial activation and dysfunction that is triggered by IFN-gamma, IL-6 and TNF-alpha. Activated endothelial cells, in turn, produce more IL-6.15 This excessive IL-6 activation leads to vascular leakage as well as activation of the complement and the coagulation cascade, leading to multiple organ dysfunction and disseminated intravascular coagulation.11,22 IL-6 increases the production of vascular endothelial grown factor, which internalizes vascular endothelial cadherin, a mayor structural protein that mediates adhesion of adjacent cells, leading to vascular leakage. The complement is also involved in increasing the permeability on endothelial cells, as IL-6 upregulates C5a receptors on endothelial cells and increases their responsiveness to C5a. IL-6 also induces tissue factor expression on the cell surface of monocytes, triggering coagulation cascade 22 (Figure 1). The pathophysiology of left ventricular (LV) dysfunction may be similar to that observed with sepsis induced and stress (Tako-Tsubo) cardiomyopathy.23 IL-6 has also been shown to weaken papillary muscle contraction.24

The mechanism(s) of neurologic involvement is poorly understood. Two mechanisms have been postulated, one based on the passive diffusion of cytokines,21 supported by the finding that high levels of IL-6 and IL-15,25 and a second one associated with trafficking of the CAR T cell in the central nervous system,21 as CAR T-cell numbers were found to be significantly higher in cerebral spinal fluid (CSF) in those patients with neurotoxicity,25 although CAR T cells were not detected in the CSF of all patients experiencing neurologic toxicities.26 Disruption of the blood-brain barrier (BBB) may also be a contributory factor,21,27 failing to protect the CSF from high concentrations of systemic cytokines.28 Of note, neurologic symptoms might occur after the peak of cytokines, especially after CAR T-cell therapy, so some authors consider neurological involvement as a separate entity, named CAR-T-cell-related encephalopathy syndrome (CRES).25 In addition, IL-6 blocking therapy also fails to reverse neurotoxicity in some individuals who are treated for CRS. Whether this is due to limited antibody penetration into the CNS due to the BBB, important roles for other cytokines or cytokine-independent mechanism is unknown.29
Some patients with severe CRS develop a clinical phenotype that resembles hemophagocytic limphohistiocytosis (HLH),9,30 a life threatening disorder characterized by severe systemic inflammation caused by excessive activation of cytotoxic CD8 T cells, macrophages and histiocytes.31 Primary HLH is caused by mutations in genes involved in cytolitic granule exocytosis, leading to depressed NK function and allowing macrophage activation to occur spontaneously.30 Excessive expression of IL-6 could lead to impaired lytic activity similar to that seen in familial HLH, which results in the excessive activation and expansion of CD8+T cells and macrophages.22
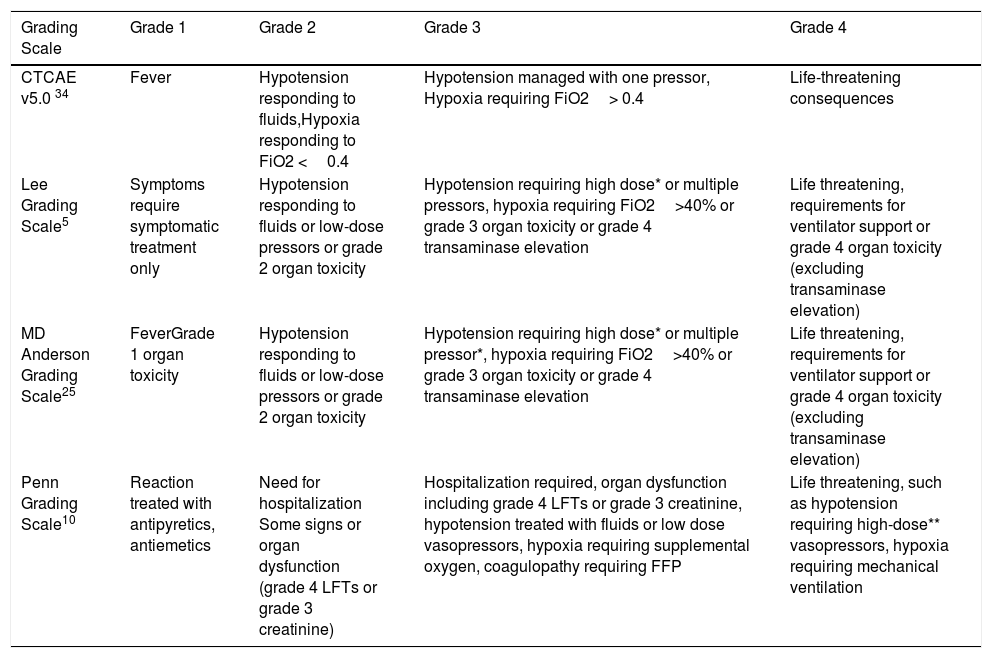
Clinical manifestationsCRS tipically manifest with constitutional symptoms, such as fever, malaise, anorexia, myalgia, headache and nausea, but can affect any organ system including cardiovascular, respiratory, skin, gastrointestinal, hepatic, renal hematological and nervous system. CRS can range in severity from low grade constitutional symptoms to a high-grade syndrome associated with severe multiorgan dysfunction (Figure 2).5,8,11,25,32,33 Several grading scales according to severity have been proposed 5,10,25,34(Table 2). Fever is a hallmark, ranging 40°C, but some patients develop CRS without fever.35 Respiratory symptoms can range from minimal dyspnea and tachypnea to severe respiratory failure, needing mechanical ventilation.5 CRS-related cardiovascular toxicity can include tachycardia, hypotension, arrhythmias, elevation in serum troponin, prolongation of the corrected QT interval, LV dysfunction and cardiopulmonary arrest.23 Neurologic symptoms and signs including confusion, delirium, aphasia, motor weakness, obtundation, myoclonus, seizure and cerebral edema have been reported.21 Diminished attention, language disturbance and dysgraphia are the earliest signs.25 Although most cases of neurological toxicity are reversible, life-threatening cerebral edema in patients treated with CAR T cells has been reported.21

CRS grading scales.
| Grading Scale | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| CTCAE v5.0 34 | Fever | Hypotension responding to fluids,Hypoxia responding to FiO2 <0.4 | Hypotension managed with one pressor, Hypoxia requiring FiO2> 0.4 | Life-threatening consequences |
| Lee Grading Scale5 | Symptoms require symptomatic treatment only | Hypotension responding to fluids or low-dose pressors or grade 2 organ toxicity | Hypotension requiring high dose* or multiple pressors, hypoxia requiring FiO2>40% or grade 3 organ toxicity or grade 4 transaminase elevation | Life threatening, requirements for ventilator support or grade 4 organ toxicity (excluding transaminase elevation) |
| MD Anderson Grading Scale25 | FeverGrade 1 organ toxicity | Hypotension responding to fluids or low-dose pressors or grade 2 organ toxicity | Hypotension requiring high dose* or multiple pressor*, hypoxia requiring FiO2>40% or grade 3 organ toxicity or grade 4 transaminase elevation | Life threatening, requirements for ventilator support or grade 4 organ toxicity (excluding transaminase elevation) |
| Penn Grading Scale10 | Reaction treated with antipyretics, antiemetics | Need for hospitalization Some signs or organ dysfunction (grade 4 LFTs or grade 3 creatinine) | Hospitalization required, organ dysfunction including grade 4 LFTs or grade 3 creatinine, hypotension treated with fluids or low dose vasopressors, hypoxia requiring supplemental oxygen, coagulopathy requiring FFP | Life threatening, such as hypotension requiring high-dose** vasopressors, hypoxia requiring mechanical ventilation |
Rarely, patients treated with BiTe 31,36 or CAR T-cells37 and severe CRS can evolve into fulminant HLH.25 This syndrome is characterized by the presence of fever, cytopenias, splenomegaly, hypofibrinogenemia, hyperferritinemia, haemophagocytosis, high levels of soluble CD25 and low NK cell activity, lymphohistiocytic tissue infiltration and multiorgan failure.38
Symptoms of CRS typically occur within 30-120minutes after infusion has been initiated,39 and typically the risk is greater during the first infusion.40 After CAR T-cell therapy, the onset of CRS symptoms seems to be dependent on the administered dose of the active agent of the proliferation kinetics of adoptively transferred cells and ranges from a few minutes up to 14 days but usually occurs within the first week.11
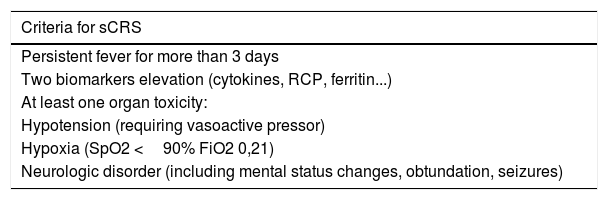
DiagnosticToxicity of these new treatments is distinct from those seen with traditional chemotherapies and we have to be aware for fast recognition. Actually there are no established diagnostic criteria for the CRS. An accurate approach included 3 items: a) compatible clinical symptoms, b) elevated biomarkers and c) recent treatment with any biological agent. As described previously the inflammatory response can manifest with low-grade or high-grade of clinical symptoms. Almost always fever, constitutional symptoms, and can evolve to hypotension, hypoxia and/or neurologic disorders.26,33 Elevated markers of inflammation such as ferritin or CRP,26 or abnormal laboratory findings indicated organ dysfunction are commonly. The severity will be determined by the intensity of the symptoms and their response to treatment (see Tables 2 and 3).
Diagnostic criteria for sCRS.
| Criteria for sCRS |
|---|
| Persistent fever for more than 3 days |
| Two biomarkers elevation (cytokines, RCP, ferritin...) |
| At least one organ toxicity: |
| Hypotension (requiring vasoactive pressor) |
| Hypoxia (SpO2 <90% FiO2 0,21) |
| Neurologic disorder (including mental status changes, obtundation, seizures) |
Circulating cytokine levels could serve as biomarkers to diagnose and potentially quantify syndrome severity but this are often costly and may not be readily available in all clinical settings. CRP is produced by the liver in response to IL-6 so serve as a reliable surrogate for IL-6 bioactivity.5,23,41 Moreover is rapid, inexpensive, can be monitoring and available in most hospitals. A combination of clinical features and biomarkers has been employed for predicting severity.10 There are ongoing investigations for determine a cytokine profile for predict severity and guide treatment 42,43 and also for establish CRP peak levels and fold change to identified patients at risk for sCRS.26,30 High risk patients should be close monitored like patients with high disease burden and comorbidities.
The syndrome can be overlapping with other pathologies simultaneously that have to be rule out. Events can appear during or shortly after first exposure to a “new” drug, so a differentiation to anaphylaxis may be difficult. There are few allergy-specific symptoms such as urticaria or glottis edema which may guide an allergic diagnosis.18,44 In a subset of patients with sCRS there is a symptom pattern similar to that seen in secondary HLH.30 Another clinical differential diagnosis is the drug-induced capillary leak syndrome (CLS), where predominates generalized edema, exudative serous cavity effusions, noncardiogenic pulmonary edema, persistent hypotension in some cases with hipovolemic shock, weight gain and acute kidney injury. Moderate to severe capillary leak syndrome are often indistinguishable from sepsis and septic shock.
PreventionTo address safety innovative strategies have been described as dual-receptor mode for engineered T cells, switch molecules for control the dose of activated CAR-T cells or insertion of suicide genes.21,45–47 Despite a lot of investigation for predicting toxicity no consensus exists on the optimal assay format to test.48 Dose fractionation, reduction of the infusion rate, corticosteroid premedication and close monitoring is the routine practice for increasing safety.
TreatmentThere is a systematic approach based on anti-IL6 therapy and corticosteroids. General precautions have been recommended by some authors.25,33 In our hospital patients remain hospitalized in general ward seven days after received CAR-T cell, and 48h for BiTe therapy. If fever appears is mandatory to assess for infection and start empiric broad-spectrum antibiotic therapy, because undiagnosed infections can have catastrophic consequences.
We recommend a four step approach (figure 3): monitoring, assessment of CRS, grading toxicity and treatment. The management of CRS have to be in accordance with the grade of toxicity. Grade 1 CRS can be managed with symptomatic treatment on the hospitalization ward. In patients with grade 2, CRS hypotension have to be promptly treated with intravenous fluid boluses. If hypotension is refractory to fluid boluses it has to be considered transfer the patient to the ICU and should be initiated anti-IL6 therapy and low-dose vasopressors. It's important that patients treated with CAR-T cell and high risk immunotherapy are managed with a multidisciplinary approach, including intensivist that should be involved from the beginning of these therapies. Bedside echocardiography and/or non-invasive hemodynamic monitoring are recommended for assess LV function.5,25 Hypoxia could be part of the syndrome and should be managed as needed, even with high flow oxygen or mechanical ventilation. It is necessary to evaluate other organ toxicities. Severe CRS, involving grades 3 and 4, or persistent grade 2 despite two doses of anti-iL6 therapy, should be treated with corticosteroids.25,35

There is a strong positive correlation with the peak IL-6 levels and the severity of the CRS.8,25,26,49 The blockage of IL-6 have became the best choice for controlling moderate-severe CRS.5,8,26,50 Tocilizumab is a MAb blocking IL-6 receptor (IL-6R). First approved for the treatment of rheumatoid arthritis 51 and in 2017 for the treatment of severe or life-threatening CAR-T cell induced CRS. The optimal dose and schedule are not well established,52 the normal dose is 8mg/kg (data generated in clinical trials). It is controversial the use of a second dose (in the next 8 to 24h) if the patient does not respond because it has a very long half-life (10-14 days). Tocilizumab has a very secure profile with few adverse effects 52 like prolonged neutropenia (probably for margination in the vessel), thrombopenya, elevation of transaminases. Siltuximab is a human-murine chimeric mAb against IL-6 and in 2014 it was FDA-approved for the treatment of multicentric Castleman's disease. Various authors have demonstrated rapid resolution, between 1 to 3 days, of the sCRS after IL-6 blockage. It is important to note that IL-6 blockade does not appear to diminish expansion of the CAR-T cells.9,26,35,52 Despite this, the current approach aims at limiting the use only for severe and life-threatening CRS because early immunosuppression could limit the efficacy of immunotherapy.5
Corticosteroids are also effective in the management of sCRS, however in the context of immunotherapy should be avoided if it's possible because suppress T-cell function and/or induce T-cell apoptosis. It has to be considered only when anti IL-6 therapy failed.25 Specially in the context of CAR-T cell therapy, because steroids reduce its clinical effectiveness by blocking T-cell activation, function and proliferation,52 and could potentially favour a recurrence of disease.26 Glucocorticoids have been shown to reduce cytokine production secondary to BiTe therapy without compromising cytotoxic T-cell proliferation and cytotoxicity.53 There is not a steroid established dose, in our center we use metilprednisolone 1-2mg/kg/day, other authors referred more elevated doses. The duration of corticosteroid treatment is determined by the resolution or improvement of symptoms.
In the onset of CRES treatment changes. Seizure prophylaxis with levetiracetam is recommended for 30 days after infusion if the CAR-T cell therapy has been associated to CRES. Status epilepticus should be managed with benzodiazepines and additional antiepileptics (levetiracetam and phenobarbital are preferred). In severe cases of CRES, seizures, motor weakness, mental obtundation and cerebral edema can occur so we recommend transfer to the ICU for frequent evaluation and monitoring with EEG and make a CT scan or RNM for discard a structural origin of the symptoms. The manifestation of CRES can be biphasic. The first phase occurs with the onset of the CRS within the first 5 days. The second phase occurs beyond 5 days, after the fever and other symptoms of CRS subside, in this case the anti-IL-6 therapy seems to be less effective, and steroids is the preferred treatment (dexamethasone 10mg/6h iv). If there is no improvement or worsening, blockage IL-6 is mandatory because there is a greater permeability of the BBB in the context of CRS enabling increased diffusion of the MAb and effective blocking IL-6.25
Other specific agents against cytokines have been used with limited results such as infliximab or etanercep. In refractory cases methylprednisolone boluses and/or cyclophosphamide for limiting CAR-T cell proliferation could be considered.
PrognosisThe global prognosis of CRS is good, more times is mild, often reversible with good response to specific treatment. Nevertheless this syndrome can be severe with life-threatening consequences and rapidly progress to a multiorgan failure. Neurologic impairment can be also reversible, but could be serious, with cerebral oedema and brain death can occur.
Another handicap is the poor prognosis of the disease itself. There can exist concerns about the indication of intensive care admission in these patients, but we should consider that we are facing patients with a potentially reversible drug related adverse event, treated with a new drug that could change the prognosis of the disease. We consider that the ICU should remain open to these patients, with the support of a multidisciplinary team involving also of oncologist and haematologist, in order to determine the intensity of treatment.
FutureIn the following years there will be an expanded use of immunotherapy in cancer 47 and due to the potential complications of these therapies, intensivist are having an important role in the management of those patients. Future studies will help to optimize patient selection, preparation, safety, and management of individuals who received immunotherapy and elucidate if potential long-term concerns as genotoxicity are valid.54
Well defined diagnostic criteria, standardized multidisciplinary treatment and determine cytokines profiles for predict severity and guide treatment are interesting topics to work on.
Conflicts of interestThe authors declare that they have no conflicts of interest.

