


In 2004 the first edition of the “Surviving sepsis campaign” guidelines for the management of severe sepsis and septic shock was published, opening a new era in the treatment of this syndrome. The paradox is that the application of these guidelines has produced positive results despite including in some cases the treatments proved ineffective. Eight years later has been published the third edition of the guides, which updates the prior in the light of new knowledge, but the quality of evidence remains weak. In this paper the authors express their critical view on the current edition of the guides, pointing out their weaknesses and suggesting how the development of future editions should be.
El año 2004 se publicó la primera edición de las guías de práctica clínica para el tratamiento de la sepsis grave y el shock séptico de la «Campaña sobrevivir a la sepsis», abriendo una nueva etapa en el tratamiento de este síndrome. Se da la paradoja de que en estos años se han producido resultados positivos aplicando medidas que en algunos casos se han demostrado ineficaces. Ocho años después se publica la tercera edición, que actualiza las previas a la luz de los nuevos conocimientos, pero la calidad de la evidencia en que se basan las recomendaciones sigue siendo insuficiente. En este documento, los autores expresan su punto de vista crítico sobre la edición actual de las guías, señalan sus puntos débiles y apuntan cómo debe ser en su opinión el desarrollo de futuras ediciones.
Clinical practice guides (CPGs) are “documents that include recommendations designed to optimize patient care, based on a systematic review of the evidence and assessment of the benefits and risks of the different options”.1 The first edition of the CPG “Surviving sepsis campaign” (SSC) for the treatment of severe sepsis and septic shock was published in the year 2004.2 This was the first time in decades in which effective treatments for sepsis seemed to have been established at last: goal-directed resuscitation,3 activated protein C,4 and hydrocortisone.5 At the same time, the importance of early antibiotic treatment in patients with septic shock became apparent.6 Above all, however, the guide offered a firm and global approach to the management of this syndrome, which up until then had only been addressed in a fragmented manner.
In 2007, a consensus document of the SEMES-SEMICYUC was published on the diagnosis and initial treatment of severe sepsis, placing emphasis on the need for multidisciplinary collaboration,7 while the second edition of the CSS guide appeared in 2008,8 for the first time basing its recommendations on the GRADE system.9 While positive and in some cases spectacular results were reported with application of the guide in individual hospitals,10,11 together with positive but not so brilliant results in large multicenter studies with a lesser degree of compliance,12,13 some doubts started to appear regarding the efficacy of the therapeutic measures on which the recommendations of the guide were based.14–17 The third edition of the SSC guide for the treatment of severe sepsis and septic shock has now been published,18 providing an update to the previous editions in the light of new knowledge.
During the last decade, the paradox has been that good results have been obtained using measures which to a considerable degree have been shown to be ineffective when evaluated individually (activated protein C, strict blood glucose control, liberal indications of hydrocortisone), or which lack a plausible physiological basis—such as the use of central venous pressure to guide fluid therapy during the resuscitation phase.19 While the recommendations dependent upon time and which require an organized approach (quantitative resuscitation, early antibiotic treatment) are maintained (albeit with an insufficient level of evidence), the more specific measures now disappear from the recommendations (activated protein C), or their indications have been amended and reduced (hydrocortisone). The key consideration in a syndrome as complex and heterogeneous as sepsis is probably the importance of the organization of medical care, rather than the particular effectiveness of the individual measures, which are inserted in a complex management plan that must be applied within a narrow time window.20 Some years ago, Pronovost wrote a very appropriate sentence that is fully applicable to the treatment of sepsis: “the greatest opportunity for improving the patient prognosis in the next 25 years will come not from the discovery of new treatments but from learning how to make more effective use of the already existing therapies”.21
It is recognized that although the recommendations are made based on the best available evidence, they cannot be regarded as a standard of treatment, because the degree of compliance (and of acceptance) of many of them by the health professionals has been12,13 and remains22 poor. Why the CPGs are not followed is a complex problem that will not be discussed here, though in the case of the SSC guidelines the main reason is probably the fact that the quality of the evidence on which they are based is insufficient; as a result, many professionals do not take them to be reliable. Another reason is that the application of these guides requires profound organizational modifications, a radical cultural change and important institutional support, which to date have not received the necessary impulse.
ValidityExcluding those targeted to the pediatric population, the current guide contains 97 recommendations divided into 23 sections, and cover very diverse aspects related to the general management of critical patients, such as mechanical ventilation, the prevention of infections, thromboprophylaxis, the prevention of digestive bleeding, or artificial nutrition. Only a third of the recommendations are directly related to the management of infection and sepsis. Each recommendation is followed by an explanatory text (rationale), and a total of 636 literature references are cited.
It had already been pointed out after the first edition of the guide that the level of evidence on which the recommendations of the SSC are based is often insufficient.23 This shortcoming has not been improved by the new guide: only 7 of the 97 recommendations are based on a high level of evidence (A), and over one-half are based on low (C), very low (D) or non-classified levels of evidence (Fig. 1). Only 17% of the recommendations regarded as “strong” (grade 1) are based on a high level of evidence. None of the 7 recommendations based on high quality evidence are specifically referred to sepsis but rather to general supportive measures, and none of the 7 recommendations of the new bundles of measures are based on high quality evidence (Table 1).

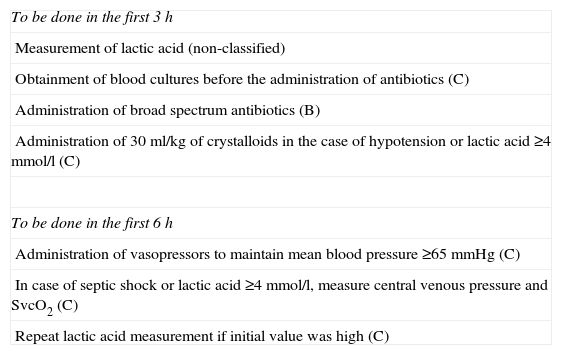
Quality of the evidence of the 7 recommendations included in the new bundle of measures.
| To be done in the first 3h |
| Measurement of lactic acid (non-classified) |
| Obtainment of blood cultures before the administration of antibiotics (C) |
| Administration of broad spectrum antibiotics (B) |
| Administration of 30ml/kg of crystalloids in the case of hypotension or lactic acid ≥4mmol/l (C) |
| To be done in the first 6h |
| Administration of vasopressors to maintain mean blood pressure ≥65mmHg (C) |
| In case of septic shock or lactic acid ≥4mmol/l, measure central venous pressure and SvcO2 (C) |
| Repeat lactic acid measurement if initial value was high (C) |
Precisely one of the reasons for the insufficient level of evidence is that many of the studies on which the general recommendations are based do not involve critical patients; as a result, their assigned level of evidence has been lowered. The lack of clinical trials exclusively involving septic patients generates noise and lessens the statistical power of the studies and their applicability to patients with sepsis.24–26
InconsistenciesAlthough it falls beyond the scope of this review to discuss the validity of the recommendations (the degree to which they fit the evidence, and the level of evidence on which they are based), it does seem questionable that the quality of the underlying evidence has not been assessed in 10 years. Moreover, the final drafting of the guide shows some inconsistencies. Several recommendations, even some considered to be “strong”, are not accompanied by any supporting literature references. Some of the recommendations are simply stated, without any explanation, and some “explanations” address issues unrelated to the recommendations they are supposed to refer to.
Some unexplained changes have been made regarding the previous recommendations: the current guide recommends a hydrocortisone dose of 200mg/day (weak recommendation) in refractory septic shock, in contrast to the previous recommendation of “up to 300mg/day”, though no reasons for this change are given. On the other hand, and with respect to the previous guidelines, the option of using fludrocortisone with hydrocortisone has been eliminated, without any explanation, and no recommendations are made on the use of etomidate for the intubation of patients with sepsis. A maximum dobutamine dose of 20μg/kg/min (strong recommendation) is advised, though without justification of this amount or references. For the initial phase of resuscitation the guide recommends (strong recommendation) a “minimum of 30ml/kg of crystalloids”, though the previous guides made no reference to this. Here again, no justification or references are given.
In our opinion, the text has some imbalances in relation to both the selected topics (e.g., the section on the prevention of infections only addresses digestive decontamination, with oral chlorhexidine—but nothing else is mentioned) and the extent to which they are discussed and referenced (some sections describe the results of clinical trials, while others do not even provide references to such studies). Only 7 tables of evidence are presented: one in the main text and 6 in the supplementary electronic material, with no clarification of the selection criteria used.
An important inconsistency of the guide, and which can lead to confusion, is the lack of concordance between the recommendation (grade 1) to administer antibiotics in the first hour following the identification of severe sepsis and septic shock, and the bundles of measures, which include the start of antibiotic treatment in the first 3h.
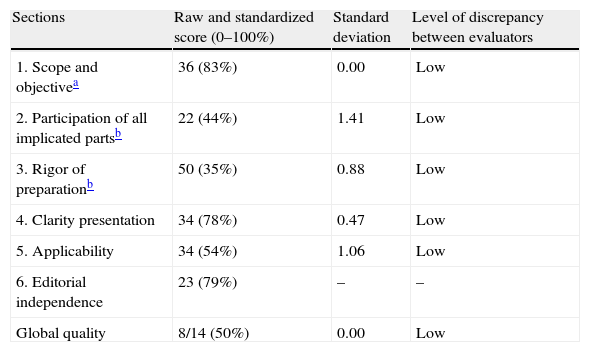
AGREE II assessmentRecently, use of the AGREE II instrument has been proposed for assessing CPGs.27Table 2 shows the results of the assessment independently made by the authors of this review in the 6 evaluated domains. We feel that the guidelines clearly have room for improvement in two of the domains: the methodological rigor used in developing and drafting them, and participation in elaboration of the guidelines. The literature search made and the study selection criteria used remain to be explained, in the same way as assessment of the quality of the recommendations (lacking in 10 of them). Likewise, it would have been better to secure a broader participation of relevant scientific societies and other elements that should be implicated in development of the guide. Future editions should make a greater effort to ensure multidisciplinary collaboration (internists, surgeons, in- and out-hospital emergency care physicians, general practitioners, nurses, health management and administrative personnel, and professional organizations)—this being an aspect that has already been addressed in this country.28 As strong points of the guide, mention must be made of the relevance of the topic dealt with, and the efforts to orientate the recommendations toward practical application—though precisely the lack of a broader participation may make this difficult. It can be concluded that in some aspects the guidelines are closer to being a “consensus conference” among experts than a CPG as defined at the start of this review.
AGREE II assessment of the “Surviving sepsis campaign” clinical practice guides.
| Sections | Raw and standardized score (0–100%) | Standard deviation | Level of discrepancy between evaluators |
| 1. Scope and objectivea | 36 (83%) | 0.00 | Low |
| 2. Participation of all implicated partsb | 22 (44%) | 1.41 | Low |
| 3. Rigor of preparationb | 50 (35%) | 0.88 | Low |
| 4. Clarity presentation | 34 (78%) | 0.47 | Low |
| 5. Applicability | 34 (54%) | 1.06 | Low |
| 6. Editorial independence | 23 (79%) | – | – |
| Global quality | 8/14 (50%) | 0.00 | Low |
Conclusion: Are these guides recommendable for use? Yes, with modifications.
The future revisions of the CPG for the management of severe sepsis and septic shock should include greater participation on the part of the implicated professionals, adopting a multidisciplinary and multinational approach, with space for participation in the development of the guide for health management and administrative personnel on one hand and patients on the other. The guidelines should be developed with the maximum methodological rigor, seeking explicit and exhaustive evidence and likewise explicit study screening and assessment criteria. Greater care also should be placed on the drafting of the recommendations, the references and explanations provided, and the presentation of the tables of evidence—ensuring complete and homogeneous consideration of all the relevant issues dealt with.
Regarding the future of the “Surviving sepsis campaign”, further quality research is needed in search of effective treatments, with increased effort focused on exploring and introducing organizational changes in the healthcare process—placing priority on the early detection of sepsis in both the out-hospital setting and in the emergency services and conventional hospital wards. To this effect we will need the firm support of the authorities and healthcare management, with promotion of the development of modern tools—especially software based systems—for the early and (where possible) automated detection of the alarm signs.
Financial supportThere have been no sources of funding.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Palencia Herrejón E, Bueno García B. Nuevas guías de práctica clínica de la «Campaña sobrevivir a la sepsis»: lectura crítica. Med Intensiva. 2013;37:600–604.

