





Double-cycling is the second most common cause of asynchrony during mechanical ventilation.1,2 Two types of double-cycling have been reported. The first one to be described is generated when vigorous and sustained inspiratory muscle effort on the part of the patient produces double cycling of the respirator.3 The second presentation, which was called false double-cycling4 and was subsequently attributed to reverse trigger (RT),5 is due to the association of a cycle started by the respirator and a subsequent cycle provoked by the patient and which generates another cycle overlapping with the previous cycle. Whether the second cycle is attributable to a reflex mechanism or not is the subject of debate, though it is probable that both types may coexist.6
Double-cycling in any form is associated to patient self-induced lung injury (P-SILI),7 whether due to RT or not, as a result of an increase in transpulmonary pressure, which generates overdistension particularly in dependent zones.8
Active expiration is a complex phenomenon regulated by pontine reflexes. The pons contains two main neuronal groups (retrotrapezoidal and parafacial) with mechanoreceptor and chemoreceptor functions. These nuclei receive information on lung volume and the level of CO2. They are activated under conditions of intense exercise, high respiratory frequency, reduced lung volume and hypercapnia. Under these conditions, they emit efferent stimuli to the abdominal muscles, generating expiratory activity,9 as an adjunct to the diaphragm and other accessory muscles.
In this letter we draw attention to a new cause of double-cycling which to the best of our knowledge has not been previously reported, where the double-cycling phenomenon is due to active expiration release associated to vigorous inspiratory muscle effort, observed during pressure support ventilation (PSV), and generating the appearance of a second effort similar to RT (PseudoRT).
The study was carried out in an obese 68-year-old woman (body mass index [BMI]: 33.21 kg/m2) admitted to intensive care in April 2020 due to COVID-19 pneumonia, and with an APACHE II score of 25. On day 31 of mechanical ventilation, monitoring was carried out during PSV of the respiratory signals as part of a study protocol on RT authorized by the Clinical Research Ethics Committee of Hospital Reina Sofía (Córdoba, Spain)(Ref.: RT-PSV 2017). Inspiratory assist 18 cmH2O over 7 cmH2O of PEEP; pH 7.31, PCO2 52 mmHg and PaO2/FiO2 142 mmHg, Vt 0.737 ± 0.048 l (13.23 ml/kg theoretical) and Fr 21.94 ± 2.44/min, mean inspiratory flow 0.83 l/s. The physical examination evidenced active expiration. Respiratory monitoring included flow, airway pressure (Paw) and esophageal (Pes) and gastric pressure (Pgas), using a multifunction esophagogastric probe (NutriVent®, Sidam, Modena, Italy); sampling at 560 Hz per channel. Multiple linear regression was used to obtain respiratory system resistances (Rrs) 17.15 cmH2O/l/s and elastance (Ers) 37.15 cmH2O/l. Transpulmonary pressure modified to transalveolar (Pt-alveolar) was calculated as: (volume*Ers)-Pes.
Monitoring showed double-cycling, together with cycles of PseudoRT appearance without double-cycling, simulating a “W” and “Stairway” image in the Pes recording. Inspiration begins with active expiration release of the preceding cycle. Following this release, vigorous muscle effort is observed, with the possible participation of inspiratory accessory muscles.
After active expiration release, a new forced expiration begins, even within the respiratory cycle, which impedes positive displacement of Pgas during diaphragm contraction. This phenomenon, expressed in terms of trans-diaphragmatic pressure, modifies the respiratory mechanics (Rrs and Ers increments). The respirator interprets the absence of active expiration as the end of inspiration, which causes early closure of the inspiratory valve. The delayed continuous and vigorous inspiratory muscle effort will provoke double-cycling or the appearance of PseudoRT without double-cycling in Paw and flow (Fig. 1).
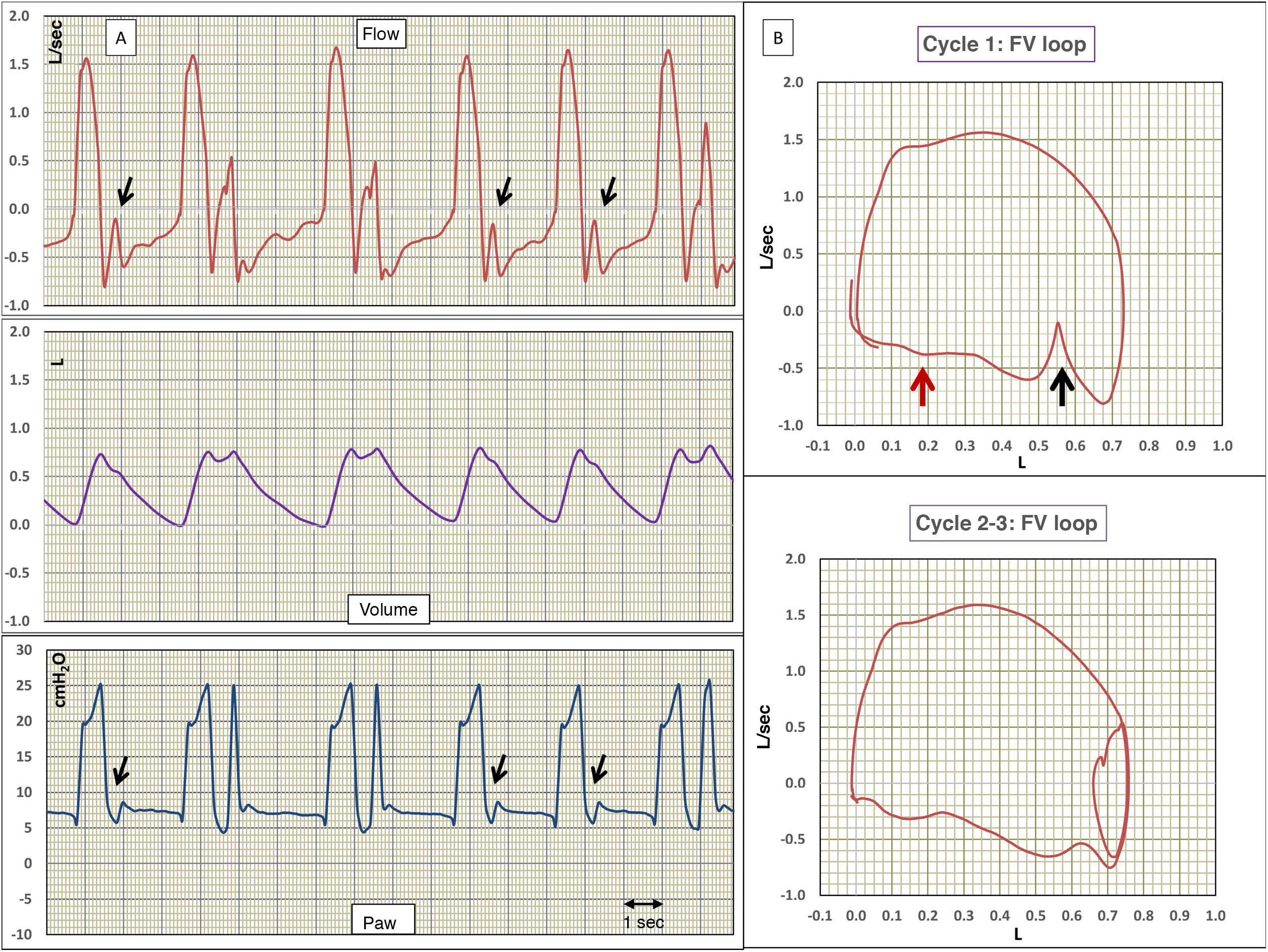
(A) Flow, volume and airway pressure (Paw) versus time. (B) Flow-volume loops (F/V). The flow and Paw signals evidence double-cycling 2–3, 3–4 and 8–9. The rest of the cycles show the usual findings of reverse trigger and/or early closure of inspiration, long vertical arrows in cycles 1, 6 and 7. The F/V loop of cycle 1 and 2–3 shows the same findings of the flow-time curve, though magnified. The loops moreover show the quite typical expiratory wavy pattern of active expiration, small red arrows.
Fig. 2 shows the real Pt-alveolar, exceeding 30 cmH2O, especially in the cycles with double-cycling, and responsible for the excessive volume – double the theoretical value for this patient. Undoubtedly, the overdistension and stretch generated favor the development of P-SILI.
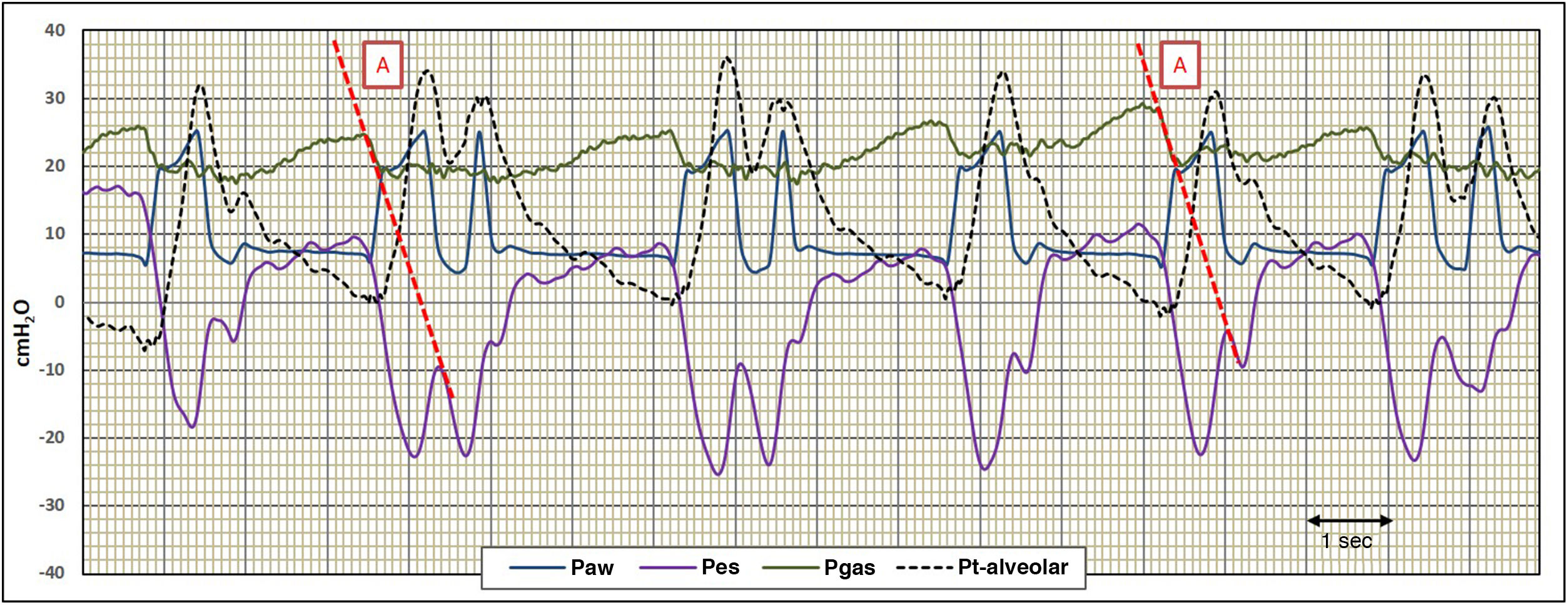
Recording of the airway (Paw), esophageal (Pes), gastric (Pgas) and transalveolar (Pt-alveolar) pressure signals. In the Pgas signal we can see the presence of active expiration, and how its release generates the start of the mechanical cycle, followed by effort of the inspiratory muscles as evidenced in Pes. The disappearance of the stimulus generated by active inspiration causes early closure of inspiration and makes the inspiratory effort more manifest, simulating reverse trigger. The vigorous effort on the part of the patient generates Pt-alveolar in excess of 30 cmH2O, causing lung overdistension and hyperinsufflation.
The present case evidences the usefulness of advanced monitoring. Without Pgas monitoring, it would not have been possible to interpret the double-cycling and apparent PseudoRT generated by the active expiration.10 Following these findings, patient sedation was increased, with a switch to assist-control mode ventilation, correcting the asynchrony, with the disappearance of forced expiration. In our opinion, the expiratory muscle activity was the gateway to abdominal-diaphragmatic discoordination.
Please cite this article as: Benítez Lozano JA, Serrano Simón JM. Pseudo reverse trigger con doble ciclado por espiración activa durante presión de soporte. Med Intensiva. 2022;46:288–289.
«In memoriam»: Dr. Benítez died on 2 June 2021, at 74 years of age, in full exercise of his functions, while the proofs of this article were being prepared. His kindness, love and inspiration, dedicated to true working spirit, progress and responsibility, have left a permanent imprint upon those of us who were at his side. The loss is irreparable, but his legacy will live on. Rest in peace.

