






To evaluate the learning of basic life support (BLS) measures on the part of laypersons after 3 different teaching programs.
DesignA quasi-experimental before–after study involving a non-probabilistic sample without a control group was carried out.
ScopePrimary school teacher students from the University of Santiago (Spain).
ParticipantsA total of 124 students (68.8% women and 31.2% men) aged 20–39 years (M=22.23; SD=3.79), with no previous knowledge of BLS, were studied.
InterventionsThree teaching programs were used: a traditional course, an audio-visual approach and feedback devices.
Main variables of interestChest compressions as sole cardiopulmonary resuscitation skill evaluation: average compression depth, compression rate, chest recoil percentage and percentage of correct compressions. Automated external defibrillator: time needed to apply a shock before and after the course.
ResultsThere were significant differences in the results obtained after 2min of chest compressions, depending on the training program received, with feedback devices having a clear advantage referred to average compression depth (p<0.001), compression rate (p<0.001), chest recoil percentage (p<0.001) and percentage of correct compressions (p<0.001). Regarding automated external defibrillator, statistically significant differences were found in Tafter (p=0.025).
ConclusionsThe teaching course using feedback devices obtained the best results in terms of the quality of chest compressions, followed by the traditional course and audio-visual approach. These favorable results were present in both men and women. All 3 teaching methods reached the goal of reducing defibrillation time.
Evaluar el aprendizaje en soporte vital básico (SVB) en personal lego tras 3 experiencias formativas diferentes.
DiseñoSe trata de un estudio cuasiexperimental antes-después de muestreo no probabilístico, sin grupo control.
ÁmbitoEstudiantes de formación de profesorado de educación primaria de la Universidad de Santiago de Compostela.
ParticipantesUn total de 124 estudiantes (68,8% mujeres y 31,2% hombres) de entre 20 y 39 años (M = 22,23; DE = 3,79), cuyo criterio de inclusión fue el no tener conocimientos previos sobre SVB.
IntervencionesSe aplicaron 3 programas formativos sobre SVB a estudiantes universitarios: curso tradicional, métodos audiovisuales y dispositivos de retroalimentación.
Variables de interés principalesEn masaje continuo: profundidad media de la compresión, porcentaje de reexpansión correcta, ratio de compresiones por minuto, porcentaje de compresiones correctas. Con el desfibrilador externo semiautomático: tiempo empleado en aplicar una descarga antes y después de la formación.
ResultadosExisten diferencias significativas en los resultados obtenidos tras 2min de masaje continuo en función de los programas formativos recibidos, favorables al método de retroalimentación: ratio de compresiones por minuto (p < 0,001), profundidad media de la compresión (p < 0,001), porcentaje de compresiones correctas (p < 0,001) y porcentaje de reexpansión correcta (p < 0,001). En cuanto al desfibrilador externo semiautomático, se encontraron diferencias estadísticamente significativas en el Tdespués (p = 0,025).
ConclusionesEl programa de formación con dispositivos de retroalimentación obtuvo los mejores resultados de calidad de compresiones cardíacas, seguido del curso tradicional y del método audiovisual. Sus superiores resultados se manifestaron tanto en hombres como en mujeres. Los 3 métodos formativos lograron el objetivo de reducir los tiempos de desfibrilación.
Sudden cardiac death (SCD) is one of the leading causes of death in industrialized countries, and more than 90% happen outside the hospital setting.1 In Europe, it is estimated that the average incidence rate of cardiorespiratory arrests (CRA) is 84% for every 100,000 inhabitants per year,2 with an average survival rate after hospital discharged of 10.3%. In Spain, back in the year 2013, there were 115,752 cases of acute coronary syndrome, of which 100,000 suffered from an acute myocardial infarction, 33% of which died before arriving to a health center.3 It is estimated that by 2021 this figure will remain stable until reaching 109,772 cases, of which 81% will be due to acute myocardial infarctions.3 On the other hand, the average response time of the emergency medical teams (EMT) is between 7 and 20min,4 based on the resources and location of the victim. According to a study conducted in the Balearic Islands, Spain, the average response time in Spain since the basic life support (BLS) is initiated by these EMTs5 is 8.3min, which is why starting the BLS maneuvers by whoever witnesses the CRA is of paramount importance here. All citizens should have some sort of basic training on how to perform cardiopulmonary resuscitation (CPR) maneuvers since they are usually the first witnesses and responders to an out-of hospital cardiac arrest (OHCA). Thus, the measures established by international ogranizations6,7 to increase the survival rates of OHCA should be observed. These measures should be oriented toward the early activation of the EMT, the performance of CPR maneuvers by first responders, early defibrillation, and further care by the advance life support team. This is even more important if we take into consideration that most OHCAs happen at the victim's own house and in public places,8–10 where the first responders can be the family members or acquaintances. This is why it is crucial that everybody knows how to initiate BLS maneuvers immediately after witnessing an OHCA, since it is of vital importance for the victim's survival.6,7,11,12 However, there is a lack of information and training when it comes to reacting to this urgent situation, and a small percentage of the population knows how to perform CPR maneuvers.13,14 Due to how difficult it is to guarantee the training of the entire population, back in the year 2015, the World Health Organization together with other international societies published a series of recommendations to teach CPR maneuvers to kids—the Hands that help-Training children is training for life initiative15 in an attempt to increase the percentage of CPR performed by witnesses—taking as an example the high rates of CPR performed by witnesses of Scandinavian countries. The initiative recommended two (2) hours of mandatory CPR training a year starting at 12 years old in schools everywhere.15
The manifest states that both healthcare professionals and teachers trained in CPR maneuvers can teach these techniques to school children, meaning that in order to meet the requirements of official BLS training in schools, teachers should be the providers of information. It is estimated that even scholars trained in CPR maneuvers15 could teach these skills to their families and friends,16 the basic skills needed to perform external chest compressions and use an automated external defibrillator (AED). This school training proposal is motivated by the fact that, at one time or another in a person's lifetime, schools are visited by nearly 100% of the population.17
So, teachers, the cornerstone of experience, should be trained, prepared, and motivated to be able to perform this task. This is why college training can increase the ratio of witnesses capable of performing CPR maneuvers.18 However, according to several reports and studies, these days, CPR is not part of the teachers’ curricula,19 which is why they do not teach CPR maneuvers to their students, because they do not have enough information on this topic, or they are not ready to deal with CPR in their classes.20,21
Due to how important it is to guarantee the best teachers’ training in BLS who, by the way should be the providers of this experience, and knowing the actual time constraints and limited resources to put it into practice, the goal of this study is to compare the degree of acquisition of the 2 fundamental skills needed to provide BLS: chest compressions, and use of AED22 in future teachers through the implementation of three (3) different short-term training methods (<1h): one traditional course; multimedia devices; and CPR feedback devices.
Material and methodsSampleA total of 124 college students from the Faculty of Teacher Training at the Universidad de Santiago de Compostela, Spain without any prior experience or training in BLS participated in this study. Those students with BLS training (CPR and use of AED) were excluded. Participation in the study was voluntary and prior written informed consent was obtained from the participants for the transfer of data and use in research. The study was approved by the bioethics committee from the Universidad de Santiago de Compostela, in full compliance with the Helsinki Convention.
Study designThe three (3) training experiences had to meet the following requirements: be designed based on the actual guidelines on the performance of CPR, last less than 60min, be a unique experience in order to avoid the possibility of confounding factors from any possible voluntary trainers, and share the same duration of limited training on a phantom to a total of 6min for every participant in shifts of continuous chest compressions of 2min each.
Once the participants had been informed and after accepting the conditions required by the research, the two factors—age and sex were recorded. After this, the participants were allocated to one (1) of three (3) study groups using the following non-randomized criterion: natural groups of class attendance. Three (3) different groups were built: one first training group using a traditional course (TGtraditional) (n=40); one second training group using multimedia resources (TGmultimedia) (n=44); and a third group (TGfeedback) (n=40) of training using one immediate feedback device for external chest compressions, plus a short explanation (<60s) on the use of AEDs.23,24
These were the training processes used:
The TGtraditional received a 40min-theory-practice course with instructor-led training in BLS and AED in groups of ten (10) people during which the importance of performing CPR maneuvers with uninterrupted chest compressions only was stressed out. On the practical side of the course, and with a ratio of one (1) instructor for every two (2) students, the participants performed external chest compression on a phantom to get used to the phantom, and with no feedback at all, and switched roles every 2min, for a total 6min-time of chest compressions per participant.
The TGmultimedia was shown two (2) short videos: one first video on external cardiac massage of chest compressions only, of 3min-and-20s duration, and a second video on how to use the AED, of 3min-and-57s duration, where an indoor soccer player suffers from a cardiac arrest and is assisted by his coach following the steps of the chain of survival. At the end of each video, one expert summarizes the key aspects of CPR for first responders. The videos are available through the following links: external cardiac massage at https://www.youtube.com/watch?v=ZQdwoRf-TLg; AED at https://www.youtube.com/watch?v=6W4zbqWWDs.20 After watching the videos, and same as it happened in the group with traditional training, the participants performed external cardiac compressions, in pairs, on a phantom and switched roles every 2min for a total 6min-time of chest compressions per participant.
The third group, TGfeedback, received a brief one-minute explanation on how to place the hands on the cardiac massage area on the feedback phantom, followed by recommendations on how to achieve the correct frequency and compression depth, while taking into consideration the teacher's indications, and the feedback from the phantom. When it comes to the AED, they received a less-than-60-s-brief explanation on how to use this device.23,24 Same as it happened with the aforementioned two training groups, the participants performed external cardiac compressions, in pairs, on a phantom and switched roles every 2min for a total 6min-time of chest compressions per participant.
After completing the training, each student was taken to a private room with a simulation including the Leardal Resusci Anne Q-CPR phantom programmed in compression mode only. Each participant was asked to perform external cardiac compressions of 2min-duration, and the results from the different parameters of the phantom program were recorded. After the two-minute massage, they were asked to use the AED on the uncovered chest of the phantom, and the time elapsed until one discharge was administered following the AED indications was recorded. The time elapsed from the moment the AED was handed out, until the students pressed the discharge button was measured, and the mistakes made while placing the patches were assessed.
ToolsOne ad hoc questionnaire was handed out in order to collect the sociodemographic data (age and sex), and prior knowledge on BLS, and those who knew or had been trained on how to perform CPR chest compressions were excluded.
One of the tools used to collect information on external cardiac compressions was the Laerdal Resusci Anne phantom using the Laerdal Skill Reporter software version 2.4. This model records the compressions and distinguishes whether they have been performed right or wrong. This whole process was conducted following the recommendations from the actual guidelines on cardiopulmonary resuscitation established by the European Resuscitation Council.7
VariablesThe following variables were collected: sex; age; average compression depth (ACD); correct reexpansion rate (CRR); compression rate per minute (CRM); and correct compressions rate (CCR). The time elapsed while applying the defibrillation with the AED before and after the training process was recorded too.
Statistical analysisQuantitative variables are expressed as mean and standard deviation (SD). Group mean analyses (ANOVA) were conducted in order to analyze any prior differences between groups in the measures of each of the variables studied. Also, bifactorial analyses of variance (ANOVA) were conducted for each of the variables studied: the group with 3 levels (traditional, multimedia, and feedback) was the first factor, while the sex variable (man–woman) was the second one. The main effects and interaction between the different variables were studied using the Bonferroni Correction to estimate significance. The statistical software IBM SPSS Statistics v. 20.0 was used. A 95% confidence interval was established (Fig. 1).
ResultsSociodemographic data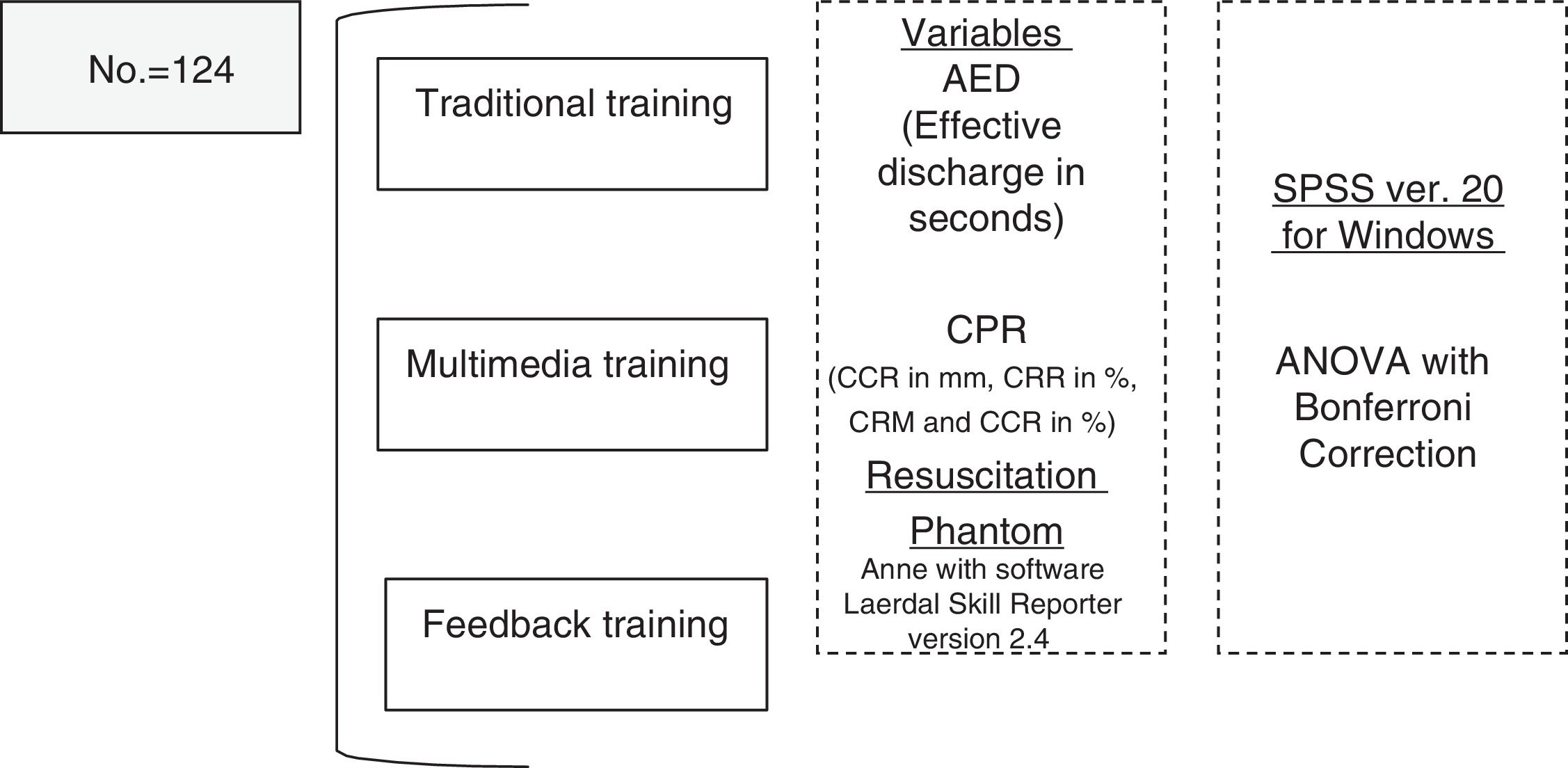
One hundred and twenty-four (124) individuals were studied (average age: between 20 and 39 years (M=22.23; SD=3.79), all of them third-year students of the Degree in Primary Education from the Faculty of Teacher Training at the Universidad de Santiago de Compostela, Spain. The traditional groups included 12 men and 28 women; the multimedia group included 12 men and 32 women, and the immediate feedback group included 14 men and 26 women. Twenty-two (22) students were excluded whether because they had former training, or some knowledge on BLS.
Times elapsed using the automated external defibrillatorTable 1 shows the means and standard deviations of the times elapsed when applying the DEA discharge before and after the training program—both overall-based, and sex-based.
Descriptive statistical analysis: variable Time in the use of AED based on sex, and overall college students.
| Variable | Men | Women | Total | Anova (Bonferroni) | ||||
|---|---|---|---|---|---|---|---|---|
| Time (s) | Program | Mean | SD | Mean | SD | Mean | SD | A vs B; A vs C; B vs C |
| Tbefore | Traditional | 63.661 | 9.861 | 69.897 | 16.404 | 68.027 | 14.775 | 0.099; 0.061; 1.000 |
| Multimedia | 61.092 | 11.132 | 62.667 | 8.574 | 62.207 | 9.165 | ||
| Feedback | 64.967 | 13.003 | 60.530 | 7.245 | 62.083 | 9.553 | ||
| Tafter | Traditional | 49.420 | 8.359 | 50.632 | 7.861 | 50.268 | 7.810 | 0.028; <0.001; 0.053 |
| Multimedia | 47.331 | 2.977 | 46.910 | 4.272 | 47.032 | 4.502 | ||
| Feedback | 43.104 | 6.327 | 44.222 | 4.272 | 43.831 | 4.946 | ||
A: traditional program: B: multimedia program; C: feedback program; SD: typical or standard deviation; s: seconds; Tbefore: time measured without training; Tafter: time measured after training based on the training program taken.
The results from the factorial ANOVA analyses conducted showed that there is a significant main effect in the training program factor F(2.118)=10.219, p<0.001, Eta2=0.148 in the time elapsed using the AED after the training period. We have not found the existence of a significant main effect in the sex factor (p=0.618), or a significant interaction between the program factor and the sex factor (p=0.751).
When it comes to paired comparisons, there is a 6.41s-difference in the application of the AED discharge (p=0.022) between women from the feedback training group, and those from the traditional training group—a tendency that can also be observed in men, with a 6.31s-difference (p<0.001). Similarly, there is a 3.90s-difference (p=0.032) between women from the multimedia training group, and those from the traditional training group. When drawing comparisons on the improvement effect—understood as the differences reported when applying a discharge between Tafter and Tbefore, no statistically significant differences among the 3 training programs were found (p=0.556): this means that this improvement is the same in the three (3) training programs, regardless of the differences seen in the times elapsed after the test.
CPR parameters recordedTable 2 shows the means the standard deviations of the parameters recorded by the skill reporter phantom after the training program, based on the training program – both overall-based, and sex-based.
Descriptive data from the variables analyzed based on chest compressions.
| Men | Women | Total | Anova (Bonferroni) | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | Program | M | SD | M | SD | M | SD | A vs B; A vs C; B vs C |
| ACD (mm) | Traditional | 49.66 | 5.71 | 43.21 | 7.06 | 45.15 | 7.26 | <0.001; 0.775; <0.001 |
| Multimedia | 45.00 | 5.32 | 30.93 | 7.84 | 35.40 | 9.69 | ||
| Feedback | 51.00 | 4.22 | 45.53 | 11.52 | 47.45 | 9.89 | ||
| CRR (%) | Traditional | 98.16 | 2.03 | 98.07 | 3.68 | 98.10 | 3.24 | 0.025; 1.000; 0.206 |
| Multimedia | 99.42 | 0.75 | 99.33 | 0.80 | 99.36 | 0.78 | ||
| Feedback | 98.71 | 1.72 | 98.38 | 1.81 | 98.80 | 1.62 | ||
| CRM | Traditional | 135.50 | 8.23 | 138.67 | 12.19 | 137.72 | 11.14 | 1.000; <0.001; <0.001 |
| Multimedia | 134.85 | 9.34 | 140.36 | 14.34 | 138.62 | 13.10 | ||
| Feedback | 116.92 | 7.86 | 119.57 | 12.05 | 118.61 | 10.74 | ||
| CCR (%) | Traditional | 46.16 | 33.86 | 25.57 | 32.00 | 31.75 | 33.52 | 0.007; 0.001; <0.001 |
| Multimedia | 29.00 | 26.13 | 4.53 | 10.31 | 12.31 | 20.27 | ||
| Feedback | 64.42 | 24.89 | 51.69 | 34.16 | 56.15 | 31.50 | ||
Mean, typical or standard deviation, based on sex and the training program taken.
A: traditional program: B: multimedia program; C: feedback program; SD: typical or standard deviation; M: mean; CCR: correct compressions rate; ACD (mm): average compression depth (mm); CRR: correct re-expansion rate; CRM: compression rate per minute.
The results from the factorial ANOVA analyses conducted on the CRM showed that there is a significant main effect of the program factor F(2.118)=31.974, p<0.001, Eta2=0.351 in the number of compression rate per minute performed on the phantom test. We have not found a significant main effect in the sex factor (p=0.098), or a significant interaction between the program factor, and the sex factor (p=0.855).
On the method of paired comparisons, we can say that both the traditional and the multimedia groups compressed the chest at an inadequate rhythm (above 120 chest compressions per minute). In the analysis conducted between men and women within each and every one of the training groups, we did not find any statistically significant differences on this regard.
The results from the factorial ANOVA analyses conducted on the ACD showed that there is a significant main effect of the program factor F(2.118)=32.204, p<0.001, Eta2=0.214 in the average compression depth on the phantom test. We found a significant main effect in the sex factor F(1.118)=17.934, p<0.001, Eta2=0.233, and, also, a significant interaction between the program factor, and the sex factor F(2.118)=3.284, p<0.041, Eta2=0.053.
On the method of paired comparisons, both men and women from the feedback training group achieve deeper depths than the other two (2) training programs. With the data obtained we can say that there is a statistically significant difference between men and women, regardless of the training program they took, on the average depth achieved (p<0.001). In the comparison drawn between men and women within the same group, we found statistically significant differences in all of them: traditional group (p=0.020); multimedia group (p<0.001), and feedback group (p=0.040).
The results from the factorial ANOVA analyses conducted on the CCR showed that there is a significant main effect of the program factor F(2.118)=20.968, p<0.001, Eta2=0.262, in the correct compressions rate on the 2-min test on the phantom. We found a significant main effect in the sex factor F(1.118)=13.202, p<0.001, Eta2=0.101, but no significant interaction between the program factor, and the sex factor (p=0.648).
On the method of paired comparisons, the participants from the feedback group achieved a higher correct compressions rate than the traditional (p=0.003) and the multimedia groups did (p<0.001). On the inter-group analysis, we found statistically significant differences between men and women from the traditional group (p=0.032), and those from the multimedia group (p=0.007).
The results from the factorial ANOVA analyses conducted on the CRR showed that there is a significant main effect of the program factor F(2.118)=3.154, p<0.046, Eta2=0.051, in the correct compressions rate on the 2-min test on the phantom. We did not find a significant main effect in the sex factor (p=0.680), or a significant interaction between the program factor, and the sex factor (p=0.966).
When it comes to the method of paired comparisons, no statistically significant differences were found within the groups when comparing men vs women.
DiscussionThe goal of this article was to verify the different training/educational methods of the BLS skill set.
The study was designed to assess three (3) teaching methods as part of one pilot experience in BLS training, and focused on eliminating confounding factors after the course, such as the material hand-out to participants, or the training that each participant could have carried out individually with such material. The organization chosen—the Faculty of Teacher Training at the Universidad de Santiago de Compostela, Spain was the target population (the future teachers) who, according to the European Resuscitation Council, should be the leading force in the teaching of CPR.15 Age differences may be a determinant factor when it comes to learning and performing CPR maneuvers; this study sample has one homogeneous average, which is why no age analysis was conducted. The three (3) training activities were conducted by personnel from the aforementioned Faculty of Teacher Training following recommendations from the “kids save lives” initiative,15 that states what the most important moment is for the acquisition of this skill set, which is why the Faculty of Teacher Training was chosen as the ideal place for the consolidation of prior skills in BLS of future teachers, or if they already had such skills, to initiate them, and guarantee training.
When it comes to defibrillation, all three (3) training methods achieved the goal of reducing the AED defibrillation times.
Out of the three (3) short-term training methods under comparison, the CPR training program with feedback devices was the one that score the best when it comes to quality of the 2-min continuous chest compressions; results that remained in the groups of both men and women. The multimedia group scored the worst when it comes to quality in the parameters analyzed during the 2-min chest compression period. In a study based on a short training of laypersons with feedback devices, González-Salvado et al., confirmed that these people scored quality ratios that were similar to those of healthcare personnel when performing chest compressions.25
With respect to other studies on this issue when it comes to teacher training few experiences have been published to date. In one of them, teachers-in-training who do not have any BLS training scored worse results in the quality of chest compression than groups from this study when they performed CPR only with chest compressions on a phantom with real time guidance from an emergency call center.26
When it comes to researches from other groups, the results obtained in our study are similar to other studies that showed that 30-min CPR seminars and courses on a personal phantom using DVDs are almost as effective as the classic 4-h courses.27 We should mention here that, in our case, this training lasted less than an hour, and the results were somehow better in the traditional training group than in the multimedia one. Thus, 1-h long trainings allow students to acquire the CPR hand skills needed,28 something that can be easily be taught at the classes.
When it comes to the multimedia training group, the results obtained were not consistent with the results coming from the actual studies that say that the results obtained in self-educational courses are the same as the ones obtained in traditional courses,29 or even help train special populations.30 We should mention here that in the actual study, we used a unique training experience under controlled training time, the same for everyone, which means that we never saw the advantages of self-educational courses, or continuous training and reinforcements, given the availability of material at the trainee's house. We share the idea that watching multimedia materials and then practicing on a phantom is the cheapest training available and allows acquiring skills similar to the skills acquired with traditional courses29 and, also, mass train young people.31,32 With this alternative, it is possible to educate populations on CPR training with a personal kit in just 30min.33
When it comes to feedback devices, the actual guidelines34 recommend that their clinical use should only be taken into consideration as a part of a wider healthcare system, that should include CPR training, since it has been confirmed that they significantly improve the ratios of spontaneous circulation in in-hospital CRAs when used in combination with a system to improve CPR through weekly training and debriefing sessions of those cases where the resuscitation maneuvers took place,35 which is consistent with what the actual study says, that they are an important piece of the puzzle in the learning of CPR skill sets.
The actual study is the first case of an educational/training plan developed in the Faculty of Teacher Training at the Universidad de Santiago de Compostela, Spain in an attempt to guarantee the training of future teachers as key participants in the training of BLS contents.15
After confirming the validity of the three (3) initial experiences and their training possibilities as a unique experience, now the strategy will be focused on new studies that will assess both the “forgetting effect” of initial experience, and the most appropriate type (self-training vs scheduled vs combined) and frequency of experience reinforcements. The goal here is to guarantee quality training for a population that is essential spreading BLS knowledge, and contribute to the implementation of the motto established by the European Resuscitation Council “community response saves lives”.36
As some of our study limitations, we should mention here that no randomization was ever conducted; nevertheless, the fact that the prior state was not knowing anything on BLS, and that the results in the most important parameters of compressions (CRA, HR, CCR) were maintained when isolating the groups into men and women, could be a plus that would be favoring homogeneous distribution. Also, it was a study conducted on a phantom, meaning that it cannot be completely generalized to the medical practice with real patients. Although the assessment of the skill set was conducted using the same conditions and times in the three (3) groups, it was an immediate post-course measure, and it was not part of the study to assess the quality of compressions after the “forgetting period”,37 which is why we do not know if, eventually, this aspect could modify long-term results. On the other hand, we should mention as well that no official materials were used to train CPR as established by the European Resuscitation Council that recommends an annual 2-hour training starting at 12 years old. Time constraints have conditioned the use of adapted materials with less training time.
ConclusionsThe training program with feedback devices scored the best quality results in the item of chest compressions, followed by the traditional course, and the multimedia method ranking last. Results that were reported in both men and women.
The three (3) training programs achieved the goal of reducing fibrillation times.
Authors’ collaborationAll authors have participated in all sections of this research and, also, in the preparation of this paper including the study idea and design, data mining, the statistical analysis, the interpretation of data, the writing of the draft, the critical review of the intellectual content, and the approval of the final version of this document.
Conflict of interestThe authors declare no conflict of interests associated with this article whatsoever, and that they have received no funding while conducting this study.
We wish to thank the college students for their altruistic participation while conducting this study.
Please cite this article as: Navarro-Patón R, Freire-Tellado M, Basanta-Camiño S, Barcala-Furelos R, Arufe-Giraldez V, Rodriguez-Fernández JE. Efecto de 3 métodos de enseñanza en soporte vital básico en futuros maestros de Educación Primaria. Un diseño cuasiexperimental. Med Intensiva. 2018;42:207–215.

